Omega-3s have become the latest “super food”. Wherever you get your news, you are constantly seeing articles about the latest “miracle results” obtained by adding omega-3s to your diet.
There is good evidence that omega-3s:
Lower blood pressure.
Reduce triglycerides (fatty particles in your bloodstream).
Reduce chronic inflammation.
Slow the buildup of plaque in the arteries (which combined with lowering blood pressure, reducing triglycerides, and reducing inflammation likely lowers heart disease risk).
Reduce the risk of depression and anxiety.
Improve neurodevelopment (cognitive function, memory, and learning) in infants and children.
Reduce inflammation in joints.
In addition, omega-3s may:
Reduce the risk of cognitive decline and Alzheimer’s as we age.
Reduce the risk of arrhythmias (irregular heartbeats).
Protect against age-related macular degeneration.
Improve immune function.
Reduce the risk of certain cancers.
Improve blood sugar regulation.
Because obesity is associated with chronic inflammation and inflammation is associated with many of the health risks associated with obesity, the authors of the study I will be describing today (J Torres-Vanegas et al. Healthcare, 13:103, 2025) decided to look at the effect of supplementation with 1.8 grams of long-chain omega-3s (fish oil capsules) on the beneficial effects of a weight loss diet in a double-blind, placebo-controlled, 8 week study.
There were two interesting wrinkles to this study.
Previous studies have suggested that a 5:1 ratio of omega-6 fats to omega-3 fats is optimal for these effects, but the typical American has an omega-6 to omega-3 ratio of between 15:1 and 20:1. So, the authors designed their study so that participants achieved a 5:1 omega-6 to omega-3 ratio.
Because short-chain omega-3s (found in plant foods) have little effect on inflammation, they were used as the “active” placebo instead of omega-6 fats.
In short, both groups received an omega-3 supplement. The “intervention” group received long-chain omega-3s from fish oil, and the “placebo control” group received short-chain omega-3s from vegetable oils (chia and flaxseed oil).
[Note: Short-chain omega-3s have many health benefits. However, their conversion to long-chain omega-3s in the human body is very inefficient, and they do not have all the health benefits associated with long-chain omega-3s.]
How Was This Study Done?
The authors of this study enrolled 40 obese (BMI≥30) adults (40% females, 60% males), aged 30-50 in a randomized, active placebo-controlled, double-blind weight loss study for 8 weeks.
The estimated caloric expenditure was determined for each participant prior to the study. Based on that estimate calories were reduced by 200 calories/day for the first 4 weeks and 400 calories/day for weeks 5-8.
Dietitians designed a recipe book of 3 main meals and 2 snacks for each day. The diets were designed to achieve the caloric restriction described above and to achieve a 5:1 ratio of omega-6 to omega-3.
Participants completed a 3-day food frequency questionnaire including 2 weekdays and 1 weekend day at the start of the study and at week 8. Participants were guided in this by a dietitian using food models to help them assess portion sizes.
Half of the participants were given a long-chain omega-3 supplement containing 1080 mg of EPA plus 720 mg of DHA (1,800 mg total) from fish oil. The other half of the participants were given a short-chain omega-3 supplement consisting of 1,600 mg of ALA from chia and flaxseed oil. The dietary assessments showed that both groups were successful in achieving a 5:1 omega-6 to omega-3 ratio when the supplements were included in the calculation.
Can Omega-3s Improve Weight Loss Diets?
Because both groups had equal caloric restriction. Therefore, as expected, both groups experienced decreased:
Body weight.
BMI.
Percent body fat.
Total cholesterol.
Triglycerides.
VLDL.
However, when the scientists measured markers of inflammation, a different picture was observed.
IL-6 (Interleukin 6) and RvD1 (resolving D1) are inversely associated with inflammation (They increase when inflammation decreases).
IL-6 and RVD1 increased only in the group supplementing with long-chain omega-3s (EPA + DHA).
IL-10 and MCP-1 (monocyte chemoattractant protein-1) are directly associated with inflammation (They decrease when inflammation decreases).
IL-10 and MCP-1 decreased only in the group supplementing with long-chain omega-3s.
These differences were highly significant.
The authors concluded, “A diet supplemented with marine n-3 (long-chain omega-3s from fish oil) improves inflammatory markers by increasing systemic levels of Resolvin D1 and IL-10 and decreasing IL-6 and MCP-1.”
“These results could provide a guide for future nutritional intervention strategies aimed to…reduce chronic low-grade inflammation by considering the omega-6 to omega-3 ratio content as a necessary calculation for a proper diet.”
[I would note that both diets achieved an omega-6 to omega-3 ratio of 5:1, but only the diet containing long-chain omega-3s reduced inflammation. So, the author’s statement is only true for long-chain omega-3s.]
In short, weight loss is known to help reduce chronic inflammation. Both groups lost weight, but only the group supplementing with long-chain omega-3s had a significant improvement in inflammatory markers.
These data suggest that supplementation with long-chain omega-3s while on a weight loss diet greatly enhances the reduction in inflammation associated with weight loss.
These data also suggest that short-chain omega-3s do not significantly reduce inflammation.
Both findings are consistent with earlier studies.
The Unexpected Benefits Of Omega-3s
The study also found that:
Abdominal obesity was reduced by 35% in the long-chain omega-3 group compared to 5.6% in the short-chain omega-3 group, and these differences were highly significant.
Weight loss for men in the long-chain omega-3 group was 9.25 pounds compared to 4.8 pounds in the short-chain omega-3 group, and these differences were significant.
Reductions in percent body fat and waist circumference were also greater for men in the long-chain omega-3 group, but these differences were not statistically significant in this small study.
In short, these data suggest that long-chain omega-3 supplementation may have enhanced weight loss. This is an intriguing finding that needs to be confirmed by future studies.
What Does This Study Mean For You?
This study is a randomized, double-blind, placebo-controlled trial, which is the gold standard for clinical studies. But it is also a very small study, so we need to carefully consider the validity of the study.
It had three major findings.
#1: Omega-3s enhance the anti-inflammatory effect of weight loss diets.
#2: This effect is only seen for the long-chain omega-3s EPA and DHA found in fish oil. The short-chain omega-3 ALA found in vegetable oils and other plant foods had no significant effect on inflammation.
The anti-inflammatory effect of long-chain omega-3s and the lack of an effect of short-chain omega-3s on inflammation are consistent with many previous studies. The only novel aspect of this study was the finding that the same effects occurred when omega-3 supplementation was added to a weight loss diet.
That is an important consideration because many weight loss diets focus on plant foods or red meats. Fish are often missing from the diet plan and long-chain omega-3 supplementation is seldom recommended.
That’s unfortunate because chronic inflammation is associated with obesity. And chronic inflammation increases the risk of heart disease, diabetes, cancer, and all the “itis” diseases. Omega-3 supplementation should be an important part of any weight loss diet.
#3: This study also suggests that long-chain omega-3 supplementation may increase the effectiveness of weight loss diets.
At this point I consider this finding as possible, but not probable. Previous studies have reported conflicting results. Some studies have suggested omega-3s aid weight loss. Others have found no effect.
We need many more studies before I would be ready to recommend omega-3 supplementation as an aid to weight loss. However, omega-3s have many proven benefits. If they also happen to make weight loss diets more effective, this would be an unexpected benefit.
The Bottom Line
A recent study looked at the effect of omega-3 supplementation during a weight loss diet. The study had three main findings.
#1: Omega-3 supplementation enhances the anti-inflammatory effect of weight loss diets.
#2: This effect is only seen for the long-chain omega-3s EPA and DHA found in fish oil. The short-chain omega-3 ALA found in vegetable oils and other plant foods had no significant effect on inflammation.
#3: This study also suggests that long-chain omega-3 supplementation may increase the effectiveness of weight loss diets.
For more information on this study and what it means for you, read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure or prevent any disease.
My posts and “Health Tips From the Professor” articles carefully avoid claims about any brand of supplement or manufacturer of supplements. However, I am often asked by representatives of supplement companies if they can share them with their customers.
My answer is, “Yes, as long as you share only the article without any additions or alterations. In particular, you should avoid adding any mention of your company or your company’s products. If you were to do that, you could be making what the FTC and FDA consider a “misleading health claim” that could result in legal action against you and the company you represent.
For more detail about FTC regulations for health claims, see this link.
Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years.
Dr. Chaney won numerous teaching awards at UNC, including the Academy of Educators “Excellence in Teaching Lifetime Achievement Award”.
Dr Chaney also ran an active cancer research program at UNC and published over 100 scientific articles and reviews in peer-reviewed scientific journals. In addition, he authored two chapters on nutrition in one of the leading biochemistry text books for medical students.
Since retiring from the University of North Carolina, he has been writing a weekly health blog called “Health Tips From the Professor”. He has also written two best-selling books, “Slaying the Food Myths” and “Slaying the Supplement Myths”. And most recently he has created an online lifestyle change course, “Create Your Personal Health Zone”. For more information visit https://chaneyhealth.com.
For the past 53 years Dr. Chaney and his wife Suzanne have been helping people improve their health holistically through a combination of good diet, exercise, weight control and appropriate supplementation.
It’s so confusing. Everyone claims they have clinical proof that their diet is the best. You will be healthier and live longer.
But the diets are so different. They range from vegan to keto. They can’t all be equally healthy. What is the truth?
To answer that question, we first need to understand how the proponents of each diet can claim theirs is the perfect diet for health and longevity. It’s because they base their claims on:
Short-term studies. Most of their claims are based on studies that range from a few weeks to a few months. You need 20- or 30-year studies to measure the effects of a particular diet on health outcomes.
Biological markers(Things like cholesterol and triglyceride levels, blood sugar control, and/or inflammation). Biological markers can predict possible health outcomes. But without long-term studies on actual health outcomes, you don’t know whether those predictions are accurate.
Comparisons with the typical American diet. Any diet looks good compared with the American diet.
Elimination of highly processed foods. While these diets emphasize different foods, they are all whole food diets. Again, any diet that eliminates processed foods is an improvement.
It doesn’t matter whether you restrict calories, restrict certain foods or food groups, or restrict the time you allow yourself to eat. You unconsciously eat less.
And when you eat less, you lose weight.
And when you lose weight, your cholesterol and triglyceride levels fall, your blood sugar control improves, and inflammation decreases.
That’s why short-term weight loss and improvement in biological markers are virtually identical with vegan and keto diets. Those diets are as different as any two diets could be. But they are both highly restrictive diets.
The take-home lesson is clear. Don’t be confused by claims based on short-term studies. What you should look for is:
Long-term studies (20 years or more)…
that look at the effect of diet on health outcomes, and…
do not compare their diet with the typical American diet.
When I first reviewed this topic 8 years ago, I could only find a few studies that met these criteria:
One study showed that people consuming primarily plant-based diets weighed less than people who consumed primarily meat-based diets for 20 years or more.
Other studies showed that people consuming primarily plant-based diets had a reduced risk of diabetes and heart disease compared to people consuming primarily meat-based diets for 20 years or more.
These are valuable observations, but they are limited. That’s why I was so excited when I came across a recent 30-year study (A-J Tessier et al, Nature Medicine, volume 31, pages 1644-1652, 2025) looking at the effect of 9 different diets on longevity and health outcomes. In short, this study looked at the effect of different diets on healthy aging.
How Was This Study Done?
The authors of this study used data from 105,015 participants in the Nurses’ Health Study (NHS) and Health Professionals Follow Up Study (HPFS). Both studies enrolled participants in 1986 and followed them through 2016. In short, they were both 30-year studies. Participants with preexisting chronic diseases were excluded from the study.
Lifestyle factors and medical histories were assessed every two years.
A detailed dietary assessment was conducted every four years. The assessments measured the intake of 152 foods. Food intakes were averaged over the duration of the study for each participant.
[Note: This study did not measure how the diets of participants changed between 1986 and 2016, although that is an interesting question. Perhaps a future study is planned.]
Based on the foods eaten, the diets of the participants were evaluated for adherence to 9 dietary patterns, which I have described in more detail below.
[Note: To be clear, the participants were not trying to follow these diets. They ate what they ate, and the investigators subsequently compared their dietary pattern with various healthy diets.]
For each of the diets included in this study, participants were divided into quintiles based on how closely their food intake adhered to the recommendations for that diet. Then the highest quintile was compared to the lowest quintile to determine how well that diet predicted “healthy aging” after a 30-year follow-up.
The term “healthy aging” was based on 5 criteria:
Longevity – achieving an age of 70 or more.
Absence of the top 11 major chronic diseases (cancer, diabetes, myocardial infarction (heart attack), coronary artery disease, congestive heart failure, stroke, Parkinson’s disease, multiple sclerosis, and ALS).
No impairment of cognitive function.
No impairment of physical health.
No mental health issues.
In other words, these were not just individuals who survived 70 years or more. They survived and thrived. They were enjoying their golden years because they still had good health and excellent quality of life.
Diets Included In This Study
The diets included in this study were:
AHEI – Alternative Healthy Eating Index (A scoring system developed by Harvard researchers to measure overall diet quality based on its ability to predict lower risks of heart attacks, strokes, and diabetes).
aMed– Alternative Mediterranean Diet Index (The aMed diet index differs from the original Med index by separating fruits and nuts into different groups, eliminating dairy, emphasizing whole grains, and excluding red and processed meats in favor of chicken and fish).
DASH – Dietary Approaches to Stop Hypertension (The name speaks for itself. But I also sometimes refer to this diet as “the Americanized version of the Mediterranean diet’ because it features foods more familiar to Americans. For example, it allows more red meat options than most of the other diets in this list.
MIND – Mediterranean-Dash intervention for Neurogenerative Delay (It is a dietary pattern designed to reduce the risk of Alzheimer’s disease and other forms of dementia. It combines elements of the Mediterranean and DASH diets but differs from both by emphasizing berries as a major fruit source, among other things.)
hPDI – Healthy Plant-Based Diet Index (It is a scoring system that measures adherence to a diet rich in healthy plant-based foods and lower consumption of less-healthy plant foods and animal foods.)
PHDI – Planetary Health Diet Index (It emphasizes foods (primarily plant foods) that are healthy and are good for the environment. Of the diets on this list, it is the most restrictive and closest to a vegan diet)
EDIH – Empirical Dietary Index For Hyperinsulinemia (It is a scoring system that measures the potential of a diet to cause chronically high insulin levels, which is associated with type 2 diabetes and certain cancers.)
EDIP – Empirical Dietary Inflammation Pattern (It is a scoring system that measures the inflammatory potential of a diet.)
UPF – Consumption of Ultraprocessed Foods (Since recent studies have shown that most Americans get between 55 and 70% of their calories from ultraprocessed foods, this is fast becoming a measure of the typical American diet.)
Note: Except for the UPF diet, these are all whole food, primarily plant-based diets.
What Diet Is Best For Healthy Aging?
Here are the results of the study (drum roll, please):
Of the 105,015 participants in this study, only 9.3% achieved healthy aging.
Adherence to any of the 8 healthy diets improved the probability of achieving healthy aging.
The odds of achieving healthy aging ranged from 1.45 for the Healthy Plant-Based Diet to 1.86 for the Alternative Healthy Eating Index.
If you were to pick one winner, it would be the Alternative Healthy Eating Index. And if you were to define healthy aging as achieving an age of 75 or more with the other 4 criteria, the odds increase to 2.24 (more than double) for the Alternative Healthy Eating Index.
As you might expect, adherence to a diet high in ultraprocessed foods had the opposite effect. It decreased the odds of achieving healthy aging by 32%.
When you look at each of the criteria for healthy aging individually, the results were a bit more nuanced:
For survival to 70+ years, the Alternative Healthy Eating Index and the Planetary Health Diet Index were tied. Both increased the odds of survival by more than 2-fold.
The Alternative Healthy Eating Index and the Planetary Health Diet Index were also tied for surviving to 70 with intake cognitive health and intact physical function.
The Empirical Dietary Index For Hyperinsulinemia edged out the Alternative Healthy Eating Index for freedom from 11 chronic diseases.
The effect of healthy diets on the odds of achieving healthy aging is independent from BMI, smoking, and physical activity. This means that:
The effects of healthy diets on healthy aging were not because people consuming healthy diets weighed less, smoked less, or exercised more.
Even if some of your lifestyle choices are suboptimal, choosing a healthy diet will increase your odds of surviving and thriving.
Finally, the study looked at the effects of individual foods on healthy aging. The results were:
Higher intakes of fruits, vegetables, whole grains, unsaturated fats, nuts, legumes, and low-fat dairy products increase your odds of healthy aging.
Higher intakes of trans fats, sodium, sugary beverages, and red or processed meats decrease your odds of achieving healthy aging.
The effects of these foods on healthy aging aren’t novel. They are consistent with dozens of other studies that have looked at the effect of individual foods on long-term health outcomes. In fact, the diets included in this study were chosen because they included foods that positively affect health outcomes and minimize foods that negatively affect health outcomes.
What About Primarily Meat-Based Diets?
I have good friends who advocate for primarily meat-based diets such as keto, paleo, and carnivore. I’m sure they are going to say, “This study is a sham. It only included primarily plant-based diets, so, of course, it is only going to show benefits for primarily plant-based diets.” I can hear their their questions now:
Why didn’t this study include any of the primarily meat-based diets? My answer is: “All the popular meat-based diets exclude one or more of the food groups associated with health and longevity and emphasize one or more of the food groups associated with a shorter, less healthy life. And these food associations are consistent among multiple long-term studies looking at the effect of various foods on health outcomes.
The authors could have constructed a similar index for each of the popular meat-based diets. But they would have been the inverse of the plant-based diet indices because the foods included and excluded from plant-based and meat-based diets are opposite. Therefore, just like the UPF index, they would have been associated with a decreased probability of achieving healthy aging.”
Why did the scientists designing this study ignore the proven health benefits of primarily meat-based diets? My answer is: “The “proven benefits” of primarily meat-based diets are based on short-term studies showing the effects of those diets on biological markers. Long-term studies looking at health outcomes are lacking.”
But modern primarily meat-based diets are a special case because they limit carbohydrates and cause ketosis. Why weren’t they included in the study? My answer is: “The Atkins diet limits carbohydrates and causes ketosis. It has been around for more than 50 years. And, to my knowledge, there are no studies showing it is beneficial long term. If the Atkins diet cannot be shown to have long-term health benefits, it is unlikely that modern diets that mimic it are healthy long term.
What Does This Study Mean For You?
The answer is clear. If you want to survive and thrive in your 70s and beyond, choose a whole food, primarily plant-based diet.
If you want the absolute best diet, follow the Alternative Healthy Eating Index recommendations. There are many online resources to guide you.
However, any whole food, primarily plant-based diet will do. The ones with the most online resources are the Mediterranean, DASH, and MIND diets. Choose the one that best fits your food preferences and lifestyle.
If you want to go more vegetarian, the Healthy Plant-Based Diet is a bit easier than a strict vegan diet.
If you are concerned about the environment, the Planetary Diet is best for you.
If you have specific health issues like hypertension, diabetes, or inflammation, there are diets designed just for you.
And if following structured diets is not your style, just:
Eat more fruits, vegetables, whole grains, unsaturated fats, nuts, legumes, and low-fat dairy products.
Eat less trans fats, sodium, sugary beverages, and red or processed meats, and ultraprocessed foods.
Finally, even if some of your lifestyle choices are suboptimal, this study shows choosing a healthy diet will increase your odds of surviving to your 70s and thriving.
The Bottom Line
A recent 30-year study looked at the effect of 8 whole food, primarily plant-based diets on healthy aging defined as:
Achieving an age of 70 or more.
The absence of the top 11 major chronic diseases.
No impairment of cognitive function.
No impairment of physical health.
No mental health issues.
The key findings were:
Adherence to any of 8 whole food, primarily plant-based diets improved the probability of achieving healthy aging.
The odds of achieving healthy aging ranged from 1.45 for the Healthy Plant-Based Diet to 1.86 for the Alternative Healthy Eating Index.
For more information on this study, why primarily meat-based diets were not considered healthy enough to be included in this study, and what this study means for you, read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure or prevent any disease.
My posts and “Health Tips From the Professor” articles carefully avoid claims about any brand of supplement or manufacturer of supplements. However, I am often asked by representatives of supplement companies if they can share them with their customers.
My answer is, “Yes, as long as you share only the article without any additions or alterations. In particular, you should avoid adding any mention of your company or your company’s products. If you were to do that, you could be making what the FTC and FDA consider a “misleading health claim” that could result in legal action against you and the company you represent.
For more detail about FTC regulations for health claims, see this link.
Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years. Dr. Chaney won numerous teaching awards at UNC, including the Academy of Educators “Excellence in Teaching Lifetime Achievement Award”. Dr Chaney also ran an active cancer research program at UNC and published over 100 scientific articles and reviews in peer-reviewed scientific journals. In addition, he authored two chapters on nutrition in one of the leading Biochemistry textbooks for medical students.
Since retiring from the University of North Carolina, he has been writing a weekly health blog called “Health Tips From the Professor”. He has also written two best-selling books, “Slaying the Food Myths” and “Slaying the Supplement Myths”. And most recently he has created an online lifestyle change course, “Create Your Personal Health Zone”. For more information visit https://chaneyhealth.com.
For the past 53 years Dr. Chaney and his wife Suzanne have been helping people improve their health holistically through a combination of good diet, exercise, weight control and appropriate supplementation.
You can’t believe everything you read on the internet. Food myths abound. And they sound so convincing. The articles you read quote clinical studies supporting their food myth. And they offer plausible sounding explanations for why their food myth is accurate.
I have written a book, “Slaying the Food Myths”, to help you recognize and avoid food myths.
I started that book by sharing “secrets only scientists” know. The top 2 are particularly relevant.
Scientists design their studies to disprove existing paradigms. That guarantees there will be studies on both sides of every issue.
Every study has its flaws. But some have more flaws (are lower quality) than others.
Unfortunately, many of the online posts you read “cherry pick” the studies that support their belief.
Some of this is innocent. The authors aren’t scientists, so they may not know the studies they quote are of low quality. While their mistake may be innocent, the information they are sharing is still wrong.
But I am less tolerant of “experts” who base their posts on studies they know are of low quality. I call them “Dr. Strangeloves”.
New food myths arise every day. And recently, food myths about seed oils have started to proliferate. Seed oils have become the latest food villain. It has gotten to the point where many people scan every label to make sure that no seed oil touches their lips.
To help clarify the situation, I have written a recent “Health Tips From the Professor” article debunking the seed oil myths.
Among the myths I discussed was the “seed oils cause inflammation” myth. In today’s “Health Tips From the Professor”, I will delve into that topic more deeply and share the latest research with you.
But before I do that, I need to return to my professor mode and share some background information.
What Are Omega-6 Fatty Acids And Why Do They Matter?
There are two classes of essential fatty acids – omega-6 and omega-3.
In each case there is a shorter fatty acid found in plant foods which is converted to a longer fatty acid which, in turn, is converted to a group of regulatory molecules that control a variety of biological functions including blood clotting and inflammation.
For the omega-6 group the shorter fatty acid is linoleic acid (LA), and the longer one is arachidonic acid (AA). Linoleic acid is the major fatty acid found in seed oils.
For the omega-3 group, the shorter fatty acid is linolenic acid, and the longer ones are EPA and DHA.
Essential fatty acids are the only foods for which it is literally true that, “You are what you eat”.
The membrane composition of every cell in your body reflects the relative amount of omega-6 and omega-3 fatty acids in your diet.
This means the ratio of omega-6 to omega-3 fatty acids in your cell membranes are identical to the ratio of omega-6 to omega-3 fats in your diet.
The significance of these statements will become apparent as I describe the study and its significance below.
What Do We Know About Omega-6 Fatty Acids And Inflammation?
This is an important question because the omega-6 fatty acid linoleic acid (LA) is the major fatty acid in seed oils. So, when someone makes the claim that seed oil causes inflammation, they are saying that omega-6 fatty acids cause inflammation. So, the question becomes, “Is that true?”
For years the answer to this question has been unclear. Some studies have concluded that omega-6 fats decrease inflammation, while other studies suggest they increase inflammation. And, of course, the influencers who warn of the dangers of seed oils have cherry picked the studies showing they increase inflammation while ignoring studies showing they decrease inflammation.
It turns out that studies claiming that omega-6 fats increase inflammation are mostly low-quality studies. So, perhaps we should ask what recent high-quality studies show.
In 2012 a systematic review of the effects of linoleic acid (LA) on inflammatory markers stated, “We conclude that virtually no evidence is available from randomized, controlled intervention studies among healthy, non-infant human beings to show that addition of LA to the diet increases the concentration of inflammatory biomarkers”.
Two major meta-analyses that pooled the data from multiple studies found that circulating LA levels were inversely correlated with cardiovascular disease and type 2 diabetes [That means that higher levels of LA correlated with lower levels of heart disease and diabetes].
A recent report from the UK Biobank study found a strong inverse association between plasma LA levels and both total and cause-specific mortality [Higher levels of LA correlated with a longer life].
Based on these and other studies, the American Heart Association concluded, “To reduce omega-6 fat intakes from their current levels [in the American diet] would be more likely to increase rather than decrease coronary heart disease.”
Clearly, recent research is trending towards the conclusion that the omega-6 fat found in seed oils reduces inflammation and the risk of major disease.
They examined the association between red blood cell membrane levels of linoleic acid (LA) and arachidonic acid (AA) and 10 biomarkers representing different phases and pathways of inflammation in a large, community-based sample (The Framingham Offspring Study).
How Was This Study Done?
The investigators used data from the Framingham Offspring Study (children of the original Framingham participants) and the Framingham Omni Cohort (a more ethnically and racially diverse population representing the current Framingham community).
There were a total of 2777 participants (mean age 66 years, 54% women, 9.8% minorities). Blood and urine samples were obtained from these participants during their scheduled examinations between 2005 and 2008.
The levels of linoleic acid (LA) and arachidonic acid (AA) were determined from red blood cell membranes.
One urinary and nine serum biomarkers of inflammation representing multiple inflammation pathways were measured. (For a list of the biomarkers tested and the rationale for their inclusion in this study, read the article.
Finally, the correlation between the omega-6 fats and biomarkers of inflammation was calculated.
Are Seed Oils Inflammatory?
The results were as follows:
Linoleic acid and arachidonic acid combined were inversely correlated with 6 biomarkers of inflammation and had no effect on the other 4.
The inverse association of linoleic acid with inflammatory biomarkers was not affected by age, gender, or ethnicity.
The authors concluded, “Our community-based study identified small, but significant, inverse associations between red blood cell linoleic and arachidonic levels and six major biomarkers of inflammation…representing a wide variety of inflammatory pathways. Our results suggest that linoleic acid is more likely to be anti- than pro-inflammatory, and the present efforts to reduce its intake are ill advised.”
Revisiting Seed Oils
Assortment Of Salad Dressing Bottles
You might be wondering what this study has to do with seed oils.
The omega-6 fat linoleic acid is a major component of seed oils (60-75%).
So, claims that seed oils are inflammatory are based on the claim that omega-6 fats are inflammatory.
This study shows omega-6 fats are more likely to be anti-inflammatory than pro-inflammatory.
Based on their heart health benefits, the American Heart Association recommends that we not decrease the amount of omega-6 fats in our diet.
Seed oils are the major source of omega-6 fats in our diet.
So, the American Heart Association recommendation about not decreasing omega-6 fats in our diet means that decreasing our use of seed oils is not a good idea.
I have debunked the other myths about seed oils in my previous “Health Tips From the Professor” article.
The only true concerns about seed oils have to do with processing, storage, and purity.
Omega-6 fats are easily oxidized, and the oxidation process can create free radicals. Free radicals can be created through high heat processing and improper storage.
Some seed oils contain undesirable impurities in their natural form. So, both the purification process and quality control testing are important.
And, as with most foods and supplements, it is “buyer beware”. Some manufacturers use the cheapest source of seed oil rather than the highest quality source.
My recommendations are:
Choose your source carefully.
For seeds and nuts look for freshness. If they look or taste funny, throw them out.
For oils and salad dressings choose reputable brands and choose ones that use low-heat processing.
Don’t overheat them.
Most vegetable oils are only suitable for use as salad dressings and other room temperature uses.
The exceptions are vegetable oils with high smoke points – for example, olive oil for stir fries and avocado oil for higher temperature cooking.
Store them safely. Don’t give them a chance to become oxidized.
We store sunflower seeds and almonds in our refrigerator and walnuts in our freezer.
We buy unsaturated vegetable oils in small quantities (so they are used up quickly) and store them in the refrigerator.
For supplements containing seed oil ingredients choose brands with high quality control standards.
The Bottom Line
Seed oils have become the latest food villain. In a recent “Health Tips From the Professor” I have debunked the seed oil myths.
In today’s article I share the latest studies showing that seed oils are more likely to be anti-inflammatory than pro-inflammatory.
For more information on this study and how to select and use seed oils safely, read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure, or prevent any disease.
My posts and “Health Tips From the Professor” articles carefully avoid claims about any brand of supplement or manufacturer of supplements. However, I am often asked by representatives of supplement companies if they can share them with their customers.
My answer is, “Yes, as long as you share only the article without any additions or alterations. In particular, you should avoid adding any mention of your company or your company’s products. If you were to do that, you could be making what the FTC and FDA consider a “misleading health claim” that could result in legal action against you and the company you represent.
For more detail about FTC regulations for health claims, see this link.
Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years. Dr. Chaney won numerous teaching awards at UNC, including the Academy of Educators “Excellence in Teaching Lifetime Achievement Award”. Dr Chaney also ran an active cancer research program at UNC and published over 100 scientific articles and reviews in peer-reviewed scientific journals. In addition, he authored two chapters on nutrition in one of the leading Biochemistry textbooks for medical students.
Since retiring from the University of North Carolina, he has been writing a weekly health blog called “Health Tips From the Professor”. He has also written two best-selling books, “Slaying the Food Myths” and “Slaying the Supplement Myths”. And most recently he has created an online lifestyle change course, “Create Your Personal Health Zone”. For more information visit https://chaneyhealth.com.
For the past 53 years Dr. Chaney and his wife Suzanne have been helping people improve their health holistically through a combination of good diet, exercise, weight control and appropriate supplementation.
You’ve seen the claims. “You should avoid all seed oils. They are toxic.”
Any time you see claims like, “Avoid all…[add the food villain of the day]” or “[a certain food] is toxic” your “truth-meter” should go on high alert. Claims like that are more likely to be hype than truth.
More specifically, the claims about seed oils are:
They are heavily processed.
They contain toxic ingredients.
They are genetically modified.
They cause inflammation and oxidative damage.
They increase your risk of inflammatory diseases, heart disease, and cancer.
A healthier option is to replace seeds oils with animal foods high in saturated fats.
Like any good food myth, there is a kernel of truth to each of these claims. In this article I will describe the kernel of truth associated with each of these claims, put them into perspective, and give practical guidelines for incorporating seed oils into your diet.
The topics I will cover are:
The truth about fats.
The truth about omega-6 fats.
The truth about saturated fats.
The truth about canola oil.
The truth about seed oils.
The Truth About Fats
The health authorities and media must think the American public is stupid. They oversimplify everything. They tell us:
Animal fats are saturated fat.
Olive oil is monounsaturated fat.
Vegetable oils are omega-6 polyunsaturated fat.
Fish oil is omega-3 polyunsaturated fat.
The truth is that every naturally occurring fat and oil is a mixture of all four kinds of fat. And each food contains a unique mixture of fats. The kernel of truth is:
Animal fats have a higher percentage of saturated fat than other fats and oils.
Olive oil has a higher percentage of monounsaturated fat than other oils.
Vegetable oils have a higher percentage of omega-6 polyunsaturated fat than other oils.
Fish oil has a higher percentage of omega-3 polyunsaturated fat than other oils.
But the full truth is that each food contains a unique mixture of fats. For example,
Meat and butter from grass-fed animals contain a greater percentage of omega-3 fats than meat and butter from animals which were fattened on corn.
Flaxseed oil has a higher percentage of omega-3 fats than other seed oils.
High-oleic sunflower oil has the highest percentage of monounsaturated fat than other seed oils.
Other vegetable oils with high monounsaturated fat content include olive oil, avocado oil, and canola oil. [Note: Although olive oil is the source of monounsaturated fat that we hear about most, avocado oil is equally high in monounsaturated fat and has a higher smoke point, which makes it a better choice for high-heat cooking.]
Walnuts have a higher percentage of omega-3 fats than other nuts.
Macadamia nuts and almonds have the highest percentage of monounsaturated fats than other nuts, with cashews and peanuts not far behind. Nut butters, of course, reflect the fat composition of the nuts.
The point I am making is that while myths are simple, the truth is much more complex.
Take Home Lesson:Every vegetable oil and every seed oil has a unique composition of fats. Each has its unique benefits and unique drawbacks.
That is something you will want to think about the next time you read an article about the dangers or the benefits of all seed oils. Every seed oil is unique. No generalization applies to all of them.
Biochemistry 101 – Essential Fats
Let’s start with the most important point.
Omega-6 fats and omega-3 fats are essential. Simply put, that means:
We can’t make them.
They are essential for life.
We must get them from our diet.
If they are essential, the next question is, “Why do we need them?” Let me start with a little “Biochemistry 101” and talk about their role in cell membranes and cellular regulation.
Cell Membranes:
You might think of cell membranes as a solid protective armor around the cells, but nothing could be farther from the truth. A better analogy would be the ocean that covers vast areas of our planet. Our membranes are quite fluid.
And that membrane fluidity is important. Our cell membranes contain receptors like the cholesterol receptor and insulin receptor that must cluster together for cholesterol and insulin to be transported into the cell. Those receptors cluster best when cell membranes are very fluid.
Our membranes are most fluid when they contain high levels of polyunsaturated fats (For membrane fluidity it doesn’t matter if they are omega-6 or omega-3). Conversely, our membranes are less fluid when they contain high levels of saturated fats.
And here is the most important point. Because our bodies cannot make omega-6 and omega-3 polyunsaturated fats, this is the one time it is literally true that, “We are what we eat”. If our diets are high in saturated fats, our membranes are high in saturated fats. If our diets are high in polyunsaturated fats, our membranes are high in polyunsaturated fats.
And the ratio of omega-6 and omega-3 polyunsaturated fats in our membranes reflects the ratio of omega-6 and omega-3 polyunsaturated fats in our diet.
Take Home Lesson: Diets high in omega-6 and/or omega-3 fats help lower cholesterol levels and improve blood sugar regulation.
Cellular Regulation:
Our cells also use the polyunsaturated fats in our cell membrane to make hormone-like substances called prostaglandins and leukotrienes that exert profound effects on nearby tissues. [Note: For the sake of simplicity, I will just talk about prostaglandins for the rest of this article, but what I say applies equally to leukotrienes.]
The enzymes that make prostaglandins do not distinguish between omega-6 and omega-3 polyunsaturated fats. They just use whatever polyunsaturated fat they come across.
That’s important because the effects of omega-6 and omega-3 prostaglandins are often different and are sometimes opposite.
Here’s where the “We are what we eat” principle comes into play. The ratio of omega-6 and omega-3s in our diet determines the omega-6 and omega-3 content of our membranes. And that determines the type of prostaglandins our cells produce.
Take Home Lessons:
Some of the benefits of omega-6s are unique because they are dependent on omega-6 prostaglandins. These benefits cannot be duplicated by diets high in omega-3s.
Because some effects of omega-6 and omega-3 prostaglandins are opposite, we need to look closely at the omega-6 to omega-3 ratio in the diet to optimize the health benefits of these two essential polyunsaturated fats.
Now, with Biochemistry 101 behind us, we are ready to look at the truth about omega-6 fats.
The Truth About Omega-6 Fats
Assortment Of Salad Dressing Bottles
Let’s start by looking at the pros and cons of omega-6 fats.
Pros Of Omega-6 Fats:
Cellular Health: Omega-6 and fats are important for maintaining proper membrane fluidity. And omega-6 prostaglandins also regulate cell metabolism and cellular repair mechanisms.
Heart Health: Omega-6s are associated with lower risk of heart disease. This is caused by:
Lower cholesterol levels due to proper membrane fluidity which allows clustering of cholesterol receptors.
More flexible endothelial cells lining our arteries, which helps lower blood pressure and prevent blockage of the arteries by blood clots. This is most likely due to more fluid cell membranes and the production of beneficial prostaglandins.
Some of these benefits are duplicated by omega-3 fats, but the American Heart Association stated in a recent Health Advisory (WS Harris et al, Circulation, 119, 902-907, 2009) that omega-6 fats are essential for some heart health benefits. They cannot be replaced by omega-3s.
Brain Health: Omega-3s get most of the press here, but experts feel that omega-6s play an important and independent role as well.
Fetal Growth and Development: Omega-6 fats are essential for normal neural development and growth. The mechanism(s) for this benefit are ill-defined.
Other Benefits:
Omega-6 fats support healthy skin, hair, and bones. The mechanisms for these effects are unknown, but most experts feel they are independent of omega-3 fats.
Omega-6 fats are also important for reproductive health. Most experts think this is due to the production of omega-6 prostaglandins.
Take Home Lesson: Omega-6 fats are essential for a healthy heart, a healthy brain, and normal fetal growth and development.
Cons Of Omega-6 Fats:
Oxidation: Omega-6 (and omega-3) fats are very susceptible to oxidation, especially at high temperatures. This can lead to free radical formation, which can promote the formation of cancer cells.
You may have seen the statement that omega-6 fats cause cancer. This is an oversimplification. A more accurate statement would be, “Improperly used, any polyunsaturated fat may increase cancer risk. But this is largely avoidable. Here are the precautions I recommend:
Choose your source carefully.
For seeds and nuts look for freshness. If they look or taste funny, throw them out.
For oils choose reputable brands and choose ones that use low-heat processing. Also, look for ones with minimal processing. They may be cloudy rather than clear, but they will also contain naturally occurring antioxidants and polyphenols.
Don’t overheat them.
Most vegetable oils are only suitable for use as salad dressings and other room temperature cooking.
The exceptions are vegetable oils with high smoke points – for example, olive oil for stir fries and avocado oil for higher temperature cooking.
Store them safely. Don’t give them a chance to become oxidized.
We store sunflower seeds and almonds in our refrigerator and walnuts in our freezer.
We buy unsaturated vegetable oils in small quantities (so they are used up quickly) and store them in the refrigerator.
Take Home Lesson: Improperly used, omega-6 fats, like any unsaturated fat, can become oxidized and form free radicals (the kernel of truth). Choose your source carefully. Don’t overheat them. Store them safely.
Inflammation: This is the one you hear the most about. You have been told that omega-6 vegetable oils (seed oils) cause inflammation. As a blanket statement, it is mostly untrue. But it does have a kernel of truth.
Let’s start with the kernel of truth:
Omega-6 fats are inflammatory only when compared to omega-3 fats. You have also been told that omega-6 fats are inflammatory when compared to saturated fats. This is false, as I will discuss below.
Let me elaborate on the first statement with a little more Biochemistry 101 (If you haven’t guessed, that’s my favorite topic. Once a professor, always a professor).
Omega-6 fats are converted into one inflammatory prostaglandin. Omega-3 fats are converted into several anti-inflammatory prostaglandins (This is an example of some omega-6 and omega-3 prostaglandins having opposite effects).
Because of their opposite effects on inflammation, some experts say that the optimal ratio of omega-6 to omega-3 fats is in the range of 1:1 to 4:1. But the typical American diet is around 15:1.
If the omega-6 to omega-3 ratio is important (and not every expert agrees that it is), the statement that we should avoid omega-6-containing vegetable oils (seed oils) because they are inflammatory is mostly untrue.
Every omega-6 oil has a different omega-6 to omega-3 ratio. For example,
Corn oil has a 50:1 ratio and sesame oil has a 42:1 ratio. If you are just going by omega-6 to omega-3 ratios, you might want to avoid these.
Soybean oil has a 7:1 ratio and extra virgin olive oil has a 5:1 ratio. They are almost in the optimal range.
Canola oil has a 2:1 ratio. It’s in the optimal range.
And flaxseed oil is the clear winner with a 1:4 ratio.
But the truth is also much more complex than you have been led to believe.
The kernel of truth is that omega-6 fats can be converted to an inflammatory prostaglandin.
But omega-6 fats can also be converted to anti-inflammatory prostaglandins. And some omega-6 fats such as GLA are anti-inflammatory.
Human clinical studies find that omega-6 fats either have no effect on inflammation or decrease it slightly (A Poli et al, International Journal of Molecular Sciences, 24, 4567, 2023).
Take Home Lesson: Omega-6 fats are converted into one inflammatory prostaglandin (the kernel of truth). But they are also converted to anti-inflammatory prostaglandins. The net effect in the human body is a slight anti-inflammatory effect.
The Truth About Saturated Fats
You have been told that saturated fats are anti-inflammatory and decrease the risk of heart disease. For many Americans those claims are enticing because it means they don’t have to change their diet. But are the claims true?
You have been told that these claims are based on science. There are clinical studies behind them. Is that true?
The problem is that there are a lot of bad studies on saturated fats in the literature, and the Dr. Strangeloves of the world cherry pick the ones that support their beliefs.
If you want to compare the effect of different kinds of fat on either inflammation or heart health, you must make sure that all other components of the diet are the same. Too many of these studies have compared a whole food diet high in saturated fat with the typical American diet high in omega-6 fats. The results are predictable. Anything is better than the typical American diet.
In a previous issue of “Health Tips From The Professor” I discussed the criteria for a good study of fats. High quality studies must:
Show the subjects stick with the new diet for the duration of the study. Subjects find it difficult to adhere to a diet to which they are not accustomed long term and often revert to their more familiar diet. This requires either very close monitoring of what the subjects are eating or measurement of fat membrane composition to verify diet adherence, or both.
Carefully control or measure what the saturated fats are replaced with. In good studies only the fat composition of the diet changes. All other components of the diet remain the same.
Last two years or more. The fats we eat determine the fat composition of our cell membranes, and that is what ultimately determines both inflammation in our bodies and our risk of dying from heart disease. While it is true to say, “We are what we eat”, changing the fat composition of our cell membranes does not occur overnight. It takes 2 years or more to achieve a 60-70% change in the fat composition of cell membranes.
Measures multiple markers of inflammation or actual cardiovascular end points such as heart attack, stroke, and deaths due to heart disease.
When studies are done that meet these criteria the results are as follows:
Inflammation (A Poli et al, International Journal of Molecular Sciences, 24: 4567, 2023):
Replacing saturated fats with omega-6 fats reduces inflammation by 8%.
Replacing saturated fats with omega-3 fats reduces inflammation by 48%
Heart Disease(FM Sacks et al, Circulation, 136, Number 3, 2017):
Replacing saturated fats with omega-6 from decreased the risk of heart disease by 24%.
Replacing saturated fats with a mixture of both omega-6 and omega-3 fats decreased the risk of heart disease by 29%. This is equivalent to statin therapy, without the side effects.
When the replacement of saturated fats with omega-6 and omega-3 fats occurred in the context of a heart healthy diet such as the Mediterranean diet, heart disease risk was reduced by 47%.
The Food and Nutrition Board of the Institute of Medicine recommends that Americans not exceed 10% of calories from saturated fat.
Two thirds of Americans exceed this limit.
The Food and Nutrition Board recommends that omega-6 fats be around 5-6% of calories. Because omega-6 fats play an important role in heart health, the American Heart Association recommends they be at 5-10% of calories.
Americans get around 6.5% of their calories from omega-6 fats.
Take Home Lesson: Replacing saturated fat with omega-6 fats reduces both inflammation and heart disease risk. Adding omega-3 fats reduces both even more. So, bringing omega-6 and omega-3 into a better balance is a good idea. But omega-6 fats are essential and are at the recommended intake for most Americans, so don’t do this by cutting back on healthy omega-6 fats. Instead, add some more omega-3s.
The Truth About Canola Oil
There are a lot of things to like about canola oil:
It is an excellent source of healthy omega-6 fats.
It has a good omega-6 to omega-3 ratio (2:1), which makes it anti-inflammatory.
It is also a good source of monounsaturated fats and has a moderate smoke point, which makes it suitable for low heat cooking.
So, why is it so unpopular? Unfortunately, it suffers from a lot of undeserved myths. Each has a kernel of truth. But like a secret passed around the room, the myths have grown with each repetition, and the truth has become unrecognizable.
So, let’s try to separate the myths from the truth.
Myth: It is genetically engineered.
Truth: It was created by old-fashioned plant breeding.
Myth: Canola oil contains toxic ingredients.
Truth:
Rapeseed oil comes from the oilseed rape plant (a relative of mustard).
Rapeseed oil contains erucic acid and glucosinolates, both of which can be toxic in large amounts (the kernel of truth).
Baldur Stefansson from the University of Manitoba bred a “double low” variety the oilseed rape plant which produces an oil that contains <2% of both erucic acid and glucosinolates and is safe for human consumption. This new oil was named canola oil (from Canada and ola for oil). This was achieved by conventional plant breeding. Not genetic engineering.
Both cultivars of the oilseed rape plant are still grown. Rapeseed oil is used for industrial purposes, and canola oil is used for human consumption.
Canola oil is tightly regulated in Canada, the US, and the EU to <2% erucic acid.
98% of the canola oil sold in the US is grown in Canada and the northern US.
Myth: Canola oil is unhealthy.
Truth: Because it is one of the least expensive omega-6 oils, canola oil is often found as an ingredient in unhealthy, highly processed, food (the kernel of truth). The solution is simple. Avoid unhealthy foods. Adding a different kind of fat to unhealthy foods is not going to make them healthier.
The Truth About Seed Oils
By now I have covered most of the myths about seed oils in my sections on omega-6 fats, saturated fats, and canola oil, but here is a quick review.
Myth: All seed oils are…[add your favorite derogatory term here].
Truth: Every seed oil has a unique composition of fats. Each has its unique benefits and unique drawbacks.
Myth: Seed oils are genetically modified.
Truth: The plants producing canola oil and high oleic sunflower oil have been modified (the kernel of truth), but they were modified by conventional plant breeding rather than genetic engineering.
Myth: Seed oils contain toxic ingredients. This myth is most often directed at canola oil.
Truth: Rapeseed oil contains components that can be toxic at high levels (the kernel of truth). However, the rapeseed plant has been bred to produce canola oil with safe levels of those components.
Myth: Seed oils are inflammatory, which increases your risk of inflammatory diseases and heart disease.
Truth: Seed oils contain omega-6 fats which can be converted into one inflammatory prostaglandin (the kernel of truth). But they are also converted to anti-inflammatory prostaglandins. The net effect in well done human clinical trials is a slight anti-inflammatory effect.
Myth: Seed oils cause oxidative damage, which increases your risk of cancer.
Truth: Seed oils (like any polyunsaturated fat) are susceptible to oxidation, especially at high temperatures. This can lead to free radical formation and oxidative damage (the kernel of truth). But this is only true when you use them improperly. The solution is to chose your source wisely, store them safely, and to not overheat them when cooking.
Myth: Saturated fats are healthier than seed oils. Replacing saturated fat with the omega-6 fats found in seed oils increases inflammation and heart disease risk.
Truth: Many studies in this area of research are poorly designed. Well-designed studies show that replacing saturated fat with the omega-6 fats found in seed oils reduces both inflammation and heart disease risk.
Myth: Omega-3 fats are healthier than the omega-6 fats found in seed oils, so we should replace seed oils with omega-3 fats.
Fact: Omega-3 fats are more effective than omega-6 fats at reducing inflammation and heart disease risk (the kernel of truth). However, omega-6 fats are essential for a healthy heart, a healthy brain, and normal fetal growth and development. We can’t make them, so we must get them from our diet. Americans are currently consuming the recommended amount of omega-6 fats. So, we should not decrease the amount of omega-6 fats in our diet. Instead, we would benefit from adding more omega-3s to our diet.
Myth: Seed oils are highly processed. High heat processing alters the oils. Processing also removes beneficial antioxidants and polyphenols from the oils.
Truth: This is mostly true. The solution is to choose your brands carefully.
For oils choose reputable brands and choose ones that use low-heat processing. Also, look for ones with minimal processing. They may be cloudy rather than clear, but they will also contain naturally occurring antioxidants and polyphenols.
It’s not easy to choose your source carefully. But this difficulty is not unique to seed oils. For example:
The term EVO is supposed to mean extra virgin olive oil was used, but cheaper oils are sometimes blended into the olive oil to save money.
If a company wishes to use the term “grass fed” on their product, they must file a certification with the USDA, but the USDA does not inspect to determine whether the certification is accurate.
Seed oils are also found as an ingredient in unhealthy, highly processed foods. The solution here is simple. Avoid unhealthy foods. Adding a different kind of fat to unhealthy foods is not going to make them healthier.
For more details about each of these Truth statements, read the article above.
The Bottom Line
There are many myths about seed oils. Each myth has a kernel of truth but is mostly false. In this week’s “Health Tips From the Professor” I discuss the myths and truths about seed oils. Because this is a complex subject, I have broken it down into individual topics that address one or more seed oil myths before talking about seed oil myths directly.
The topics I covered are:
The truth about fats.
The truth about omega-6 fats.
The truth about saturated fats.
The truth about canola oil.
The truth about seed oils.
For more details read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure or prevent any disease.
My posts and “Health Tips From the Professor” articles carefully avoid claims about any brand of supplement or manufacturer of supplements. However, I am often asked by representatives of supplement companies if they can share them with their customers.
My answer is, “Yes, as long as you share only the article without any additions or alterations. In particular, you should avoid adding any mention of your company or your company’s products. If you were to do that, you could be making what the FTC and FDA consider a “misleading health claim” that could result in legal action against you and the company you represent.
For more detail about FTC regulations for health claims, see this link.
Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years.
Dr. Chaney won numerous teaching awards at UNC, including the Academy of Educators “Excellence in Teaching Lifetime Achievement Award”.
Dr Chaney also ran an active cancer research program at UNC and published over 100 scientific articles and reviews in peer-reviewed scientific journals. In addition, he authored two chapters on nutrition in one of the leading biochemistry text books for medical students.
Since retiring from the University of North Carolina, he has been writing a weekly health blog called “Health Tips From the Professor”. He has also written two best-selling books, “Slaying the Food Myths” and “Slaying the Supplement Myths”. And most recently he has created an online lifestyle change course, “Create Your Personal Health Zone”. For more information visit https://chaneyhealth.com.
For the past 45 years Dr. Chaney and his wife Suzanne have been helping people improve their health holistically through a combination of good diet, exercise, weight control and appropriate supplementation.
Does it feel like a war is going on in your belly every time you eat? It could be IBD (inflammatory bowel disease). IBD can take several forms, but the two most common are Crohn’s disease and ulcerative colitis.
What do we know about IBD?
The symptoms of IBD can make you miserable. They include:
Abdominal pain and cramping.
Diarrhea with occasional bouts of constipation.
Gas and bloating.
Loss of appetite and/or unexpected weight loss.
There are about 1.6 million Americans with IBD and 70,000 new cases/year.
The prevalence of IBD in the United States has increased by 34% between 2006 and 2016.
As you might suspect from its name, IBD is a chronic inflammation of the gastrointestinal tract.
It is thought to be caused by “dysbiosis of the gastrointestinal track” (In layman’s terms that means damage to your intestine caused by too many bad bacteria and not enough good bacteria).
There is also a genetic component to the disease. Some people are much more susceptible to IBD than others.
If you watch TV, you know that there are drugs for treating IBD. The ads make them sound like miracle drugs. But if you listen carefully, you also know that these drugs have a long list of side effects. And some of the side effects are pretty scary.
Are There Natural Approaches For Controlling IBD?
So, if your belly is a bit rumbly, you might be wondering if there is a more natural approach you could take. We know that diet affects the balance between bad and good bacteria in our intestine. Could something as simple as changing your diet, quell the fire in your belly?
While the answer seems obvious, it has been hard to prove. The results of previous studies have been inconclusive. That is because previous studies:
Included too few people. 1.6 million people in the US with IBD may sound like a lot, but that represents only 0.4% of the population. Unless you have a really big study, there won’t be enough people who develop IBD to give you statistically significant results.
Were too short. IBD doesn’t develop overnight.
Did not include a diverse enough population. Previous studies were confined to individual countries or specific regions within a country.
This study (N Narula et al, British Medical Journal, 2021;374:n1554) was designed to overcome the limitations of previous studies. It also looked at the effect of diet on IBD from a different perspective than most previous studies.
It did not focus on the effect of individual foods on IBD. Since consumption of processed foods is known to affect the population of intestinal bacteria, the authors of this study asked whether processed food consumption might influence the likelihood of developing IBD.
How Was The Study Done?
The authors of this study used data collected from the PURE (Prospective Urban Rural Epidemiology) study between January 1, 2003, and December 31, 2016. The PURE study collected data from a very diverse population. Specifically, it collected data from 21 low-, middle-, and high-income countries across 7 geographical regions (Europe, North America, South America, Africa, Middle East, South Asia, Southeast Asia, and China).
This study followed 116,087 adults aged 35-70 years (average age 50, percent women = 60%) in the PURE study for an average of 9.7 years. During that time, 467 participants (0.4%) developed IBD.
All participants filled out a baseline food-frequency questionnaire that had been designed and validated for foods specific to their country.
Participants were asked if they had a diagnosis of Crohn’s disease or ulcerative colitis as part of an annual follow-up questionnaire. To assure the accuracy of these answers they were validated with medical records whenever possible.
Does Processed Food Give You Gas?
Does processed food give you gas? Does it give you abdominal pain, diarrhea, and bloating? In short, does it give you IBD? That is the question this study was designed to answer. Here are the results of the study:
When comparing those eating the most processed food (≥5 servings/day) to those consuming the least (≤1 serving/day), processed food consumption increased the risk of developing IBD by 1.82-fold. This finding was equally true for:
Both Crohn’s disease and ulcerative colitis.
Adults <50 and adults >50.
Every region of the world included in the PURE study.
When the investigators looked at different categories of processed foods:
Processed meat intake increased the risk of IBD by 2.07-fold.
Soft drink intake increased the risk of IBD by 1.94-fold.
Refined sweetened food intake increased the risk of IBD by 2.58-fold.
Salty food and snack intake increased the risk of IBD by 2.06-fold.
When the investigators looked at different categories of unprocessed foods:
White meat, red meat, dairy, starchy foods, fruits, vegetables, and legumes had no effect on the risk of developing IBD.
Sodium intake (as measured by urinary excretion of sodium) also had no effect on the risk of developing IBD.
Why Does Processed Food Give You Gas?
You may be wondering why does processed food give you gas – and other symptoms of IBD.
The simplest explanation is that whole grains, unprocessed fruits & vegetables, and legumes provide the fiber that supports the growth of friendly gut bacteria. Processed foods displace these foods from our diet.
But these investigators think something else about processed foods may be contributing to the increased risk of IBD. That is because in their study:
Processed meat increased the risk of IBD, but unprocessed white and red meat had no effect on IBD.
Processed sweetened foods increased the risk of IBD, but unprocessed starchy foods and naturally sweet fruits had no effect on IBD.
Processed salty foods and snacks increased the risk of IBD, but sodium intake had no effect on IBD.
The investigators also noted that in mouse studies:
Some food additives found in processed foods cause bacteria to stick to the epithelial lining of the intestine and/or cause leaky gut syndrome, both of which can lead to chronic inflammation of the intestine.
The investigators concluded, “In this study, higher ultra-processed food intake was associated with a higher risk of IBD.”
They went on to say, “As white meat, unprocessed red meat, dairy, starchy foods, fruits, vegetables, and legumes were not found to be associated with development of IBD, this study suggests that it may not be the food itself that confers this risk but rather the way the food is processed or ultra-processed…Further studies are needed to identify specific potential contributing factors among processed foods that might be responsible for the observed associations in our study.”
[Note: This is a fancy way of saying that the detrimental effects of processed foods may be due to more than the fact that they displace healthier foods from the diet. It may also be due to the effect of food additives on the risk of developing IBD.]
What Does This Study Mean For You?
IBD is a rare disease (0.4% of the population). If you don’t have digestive issues, it would be easy to ignore this study and continue with a diet of highly processed foods.
However, I would remind you that in recent issues of “Health Tips From the Professor”, I have shared recent studies showing that highly processed foods increase your risk of:
And these studies are just the tip of the iceberg. We know that diets rich in whole grains and unprocessed fruits and vegetables decrease the risk of heart attack, stroke, and Alzheimer’s disease. And a diet rich in whole grains, fruits, and vegetables is the antithesis of a processed food diet.
The evidence is overwhelming. Highly processed foods may be convenient and tasty. But if you value your health, they are not your friends.
The Bottom Line
A recent study looked at the effect of consuming processed foods on the risk of developing inflammatory bowel disease (IBD). The study found:
When comparing those eating the most processed food (≥5 servings/day) to those consuming the least (≤1 serving/day), processed food consumption increased the risk of developing IBD by 1.82-fold. This finding was equally true for:
Both Crohn’s disease and ulcerative colitis.
Adults <50 and adults >50.
Every region of the world included in the study.
The investigators concluded, “In this study, higher ultra-processed food intake was associated with a higher risk of IBD.”
They went on to say, “…This study suggests that it may not be the food itself that confers this risk but rather the way the food is processed or ultra-processed…Further studies are needed to identify specific potential contributing factors among processed foods that might be responsible for the observed associations in our study.”
[Note: This is a fancy way of saying that the detrimental effect of processed foods may be due to more than the fact that they displace healthier foods from the diet. It may also be due to the effect of food additives commonly found in processed foods on the risk of developing IBD.]
For more details on the study and what it means for you, read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure, or prevent any disease.
I don’t usually report on studies done in mice, but this study sheds light on a particularly puzzling question: Why is fructose bad for us?
The studies are clear-cut. High fructose consumption is associated with inflammation, obesity, non-alcoholic liver disease, insulin resistance, type 2 diabetes, kidney disease, increased LDL cholesterol and triglycerides, and heart disease. Based on these associations, fructose appears to be deadly. Why would anyone want to consume it?
Yet fructose is found in virtually every fruit. In fact, fructose, also known as fruit sugar, was first isolated from fruits. Hence the name fructose. Humans have been eating fruits safely for thousands of years. Fruits are very good for us. That raises the question: “If fruits are good for us, how can fructose be bad for us?”.
An important clue can be found by looking at what the food industry has done to the American diet. Because fructose imparts a pleasurable, sweet taste to foods the food industry keeps adding it to more and more foods. As a result, dietary intake of fructose has increased 100-fold over the past two centuries. It has reached the point where fructose now accounts for almost 10% of the caloric intake in the United States.
Is It The Sugar, Or Is It The Food?
Let me expand the discussion by using a couple of graphics I developed for my book, “Slaying The Food Myths”
There Are No Sugar Villains. There Are No Sugar Heroes:
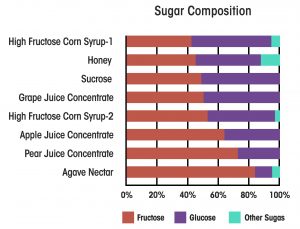
Virtually all sweeteners are primarily a mixture of fructose and glucose. The graphic on the left compares high fructose corn syrup (the current villain) with other “natural” sweeteners used in foods (our current heroes). High fructose corn syrup ranges from about 40% fructose to 55% fructose. The exact percentage depends on what kind of food product is being made with it.
Honey and coconut sugar are about 45% fructose. Sucrose and grape juice concentrate are around 50% fructose. Apple juice concentrate is around 60% fructose, and agave sugar comes in at a whopping 80% fructose.
In other words, if fructose is the culprit that everyone makes it out to be, “healthy” sugars are no better than high fructose corn syrup. Simply substituting a “healthy” sugar for high fructose corn syrup is unlikely to provide any meaningful benefit.
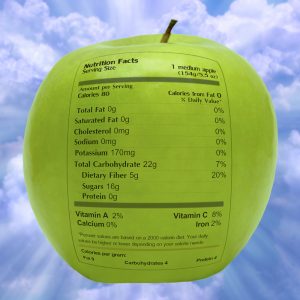
Is It The Sugar, Or Is The Food?
This graphic shows us what a nutrition label would look like on a medium apple. I am sure that label is a wake-up call for many of you. The amount of sugar and the percentage of fructose and glucose are about the same as in an 8-ounce soda sweetened with high fructose corn syrup. The same is true for virtually every other fruit you can think of.
Now let me share one more thing you won’t hear from what I refer to as “Dr. Strangelove’s Health Blog” (You probably know the ones I am referring to). Virtually all the studies showing the bad effects of fructose consumption have been done with sodas and sugary junk foods. They haven’t been done with apples.
In fact, virtually every study looking at fruit and vegetable consumption has shown they are incredibly good for us. They lower inflammation and reduce the risk of obesity, diabetes, heart disease, and cancer. And the more the better. One study found that the health benefits of fruit and vegetable consumption topped out at around 10 servings a day.
With this background, you should now fully understand why the question “If fruits are good for us, how can fructose be bad for us?” is so perplexing.
My simplistic explanation has always been that whole foods like fruits have fiber, which slows the absorption of fructose from the intestine. Our bodies were designed to handle fructose in a safe manner when it enters the bloodstream slowly. It is taken up by the liver, converted to glucose, and then slowly metered back into the bloodstream. This provides our brain and other tissues with the glucose they need for energy without blood sugar spikes. This is how fructose is supposed to be metabolized by our bodies.
Sodas and junk foods, on the other hand, have little to slow the absorption of fructose. When lots of fructose enters the bloodstream rapidly, our “safe” metabolic pathways for handling it are overwhelmed, and it is forced into the pathways that are harmful. For example, the “excess” fructose is converted to fat by the liver, which causes inflammation, obesity, fatty liver disease, and triglyceride production.
This is, of course, simply my hypothesis for explaining the different effect of fructose in fruits and sodas. It is based on sound metabolic principles, but it is far from proven. That is why I found a recent study (C. Jang et al, Cell Metabolism, 27: 351-361, 2018) so interesting. It provides a metabolic rationale for my hypothesis.
How Was The Study Done?
Mice were fed a 1:1 mixture of fructose and glucose at doses that approximated the ranges of typical human fructose consumption. The fructose was isotopically labeled so that fructose and its metabolites could be identified by LC-MS (liquid chromatography – mass spectrometry). After feeding the mice the labeled fructose, the investigator measured the amount of fructose and its metabolites in various organs and in the portal vein, which transports sugars from the intestine to the liver for additional metabolism before they enter the bloodstream.
Is Fructose Bad For You?
The first surprise was that most of the fructose was metabolized by the intestinal mucosal cells that line the small intestine rather than the liver. Previous reports had assumed that fructose was primarily metabolized by the liver because that was where most of the bad effects of fructose metabolism had been observed.
These investigators observed that fructose was primarily converted to glucose and small molecular weight metabolites by the intestinal mucosal cells before being released into the portal vein, where they were transported to the liver. However, there was a strong dose response effect.
At low fructose doses, 90% of fructose was metabolized by intestinal mucosal cells before being released to the liver.
At high fructose doses, only 70% of fructose was metabolized by intestinal mucosal cells.
That means at high fructose doses the amount of fructose reaching the liver unchanged increases from 10% to 30%. That is a 3-fold increase!
The authors concluded:
“Based on these findings, we propose that the small intestine shields the liver from fructose and that excessive doses of fructose overwhelm the small intestine, spilling over to the liver where they cause toxicity.”
“A key difference between the health effects of fiber-rich fruits (and perhaps even fiber-rich prepared foods) and juices/sodas is their rate of intestinal fructose release.”
“It is likely that the appearance rate of free fructose in the small intestine plays a critical role in dictating its metabolic fate. Like the lower doses in our experiments, a slower rate of fructose appearance will result in more complete intestinal clearance, whereas higher doses and faster rates result in fructose overflow to the liver.”
This study needs to be confirmed, and the mechanism may be entirely different in humans. However, whether mechanism is the same in mice and humans is immaterial. We already know that fructose in sodas and junk foods exerts a very different effect on our health than fructose in fruits and other fiber-containing foods.
Despite what Dr. Strangelove tells you, fructose is not bad for you. It isn’t the problem. It is sodas and junk foods containing high-fructose corn syrup that are the problem. And substituting other sugars for high-fructose corn syrup doesn’t make them any better. As I showed you above, the so called “healthy” sugars are chemically and biologically indistinguishable from high-fructose corn syrup.
The Bottom Line
Previous studies have clearly shown that fructose in sodas and junk foods is bad for us, while fructose in fruits is good for us. A recent study in mice provides a metabolic explanation for this difference. The study found:
At low fructose doses, 90% of fructose was metabolized by intestinal mucosal cells before being released to the liver.
At high fructose doses, only 70% of fructose was metabolized by intestinal mucosal cells.
That means at high fructose doses the amount of fructose reaching the liver unchanged increases from 10% to 30%. That is a 3-fold increase!
The authors concluded:
“Based on these findings, we propose that the small intestine shields the liver from fructose and that excessive doses of fructose overwhelm the small intestine, spilling over to the liver where they cause toxicity.”
“A key difference between the health effects of fiber-rich fruits (and perhaps even fiber-rich prepared foods) and juices/sodas is their rate of intestinal fructose release.”
“It is likely that the appearance rate of free fructose in the small intestine plays a critical role in dictating its metabolic fate. Like the lower doses in our experiments, a slower rate of fructose appearance will result in more complete intestinal clearance, whereas higher doses and faster rates result in fructose overflow to the liver.”
This study needs to be confirmed, and the mechanism may be entirely different in humans. However, whether mechanism is the same in mice and humans is immaterial. We already know that fructose in sodas and junk foods exerts a very different effect on our health than fructose in fruits and other fiber-containing foods.
Despite what Dr. Strangelove tells you, fructose is not bad for you. It isn’t the problem. It is sodas and junk foods containing high-fructose corn syrup that are the problem. And substituting other sugars for high-fructose corn syrup doesn’t make them any better. As I showed you above, the so called “healthy” sugars are chemically and biologically indistinguishable from high-fructose corn syrup.
For more details, read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure, or prevent any disease.
Inflammation is a bit like Dr. Jekyll and Mr. Hyde. Acute inflammation plays a valuable role in our immune response. But chronic inflammation is a scourge. Chronic inflammation:
Is a key component of all the “itis” diseases.
Can lead to autoimmune diseases.
Is thought to play an important role in heart disease.
Is associated with many other diseases, such as diabetes, cancer, Alzheimer’s disease, and inflammatory bowel diseases (IBS).
While there are many causes of chronic inflammation, diet plays an important role. In a previous issue of “Health Tips From the Professor” I have described how an anti-inflammatory diet can quell the fires of chronic inflammation.
Fiber from unprocessed plant foods is a key component of an anti-inflammatory diet. But are all plant fibers equally effective at reducing inflammation? Here is what we know:
Fiber from whole grains, vegetables, and fruits have different chemical and physical characteristics and support the growth of different species of friendly bacteria in our intestines.
Previous studies have shown that higher intakes of dietary fiber are associated with lower risk of heart disease.
Studies have suggested that fiber from whole grains may be more effective than fiber from fruits and vegetables at reducing heart disease risk.
Chronic inflammation is highly associated with the development of heart disease. This has led to the hypothesis that fiber from whole grains may be more effective than other plant fibers at reducing chronic inflammation.
Some studies have supported this hypothesis, but they have all been done with middle-aged participants, not with elderly participants who characteristically have higher levels of inflammation.
Test the hypothesis that whole grain fiber is more effective than vegetable or fruit fiber at reducing inflammation.
Determine how important reducing inflammation is at reducing the risk of heart disease.
Extending these findings to an older population group.
How Was The Study Done?
The data for this study was obtained from the Cardiovascular Health Study (CHS), a study designed to characterize factors influencing cardiovascular health in American adults aged 65 years or older. This study analyzed data from 4,125 participants (40% men, 95% white) who enrolled in the CHS study from 1989 to 1990.
These participants did not have heart disease at the time they were enrolled in the study. They had an average age of 72.6 at the beginning of the study and were followed for an average of 11.9 years. During that time 1,941 (47%) of them developed heart disease.
When the participants were enrolled in the study:
A food frequency questionnaire was administered to them by a trained dietitian to assess their long-term usual dietary intake. This information was used to assess:
Their total fiber intake and…
Their fiber intake from various dietary sources (whole grains, vegetables, and fruits).
Fasting blood samples were collected and used to analyze various markers of inflammation.
A follow-up via phone was conducted every 6 months to track an initial diagnosis of cardiovascular disease.
At the end of the study, the investigators analyzed:
The effect of total fiber and fiber from different food sources on the risk of developing heart disease.
The effect of total fiber and fiber from different food sources on inflammatory markers in the blood.
The extent to which decreased inflammation could explain the effect of whole grain fiber on reducing heart disease.
Do Whole Grains Reduce Inflammation?
With respect to inflammation:
Increased intake of total fiber was associated with healthier levels of the inflammatory markers CRP, IL-1RA, and sCD163.
Increased intake of fiber from whole grains was associated with healthier levels of the inflammatory markers CRP, IL-6, and IL-1RA.
Increased intake of vegetable fiber was not significantly associated with healthier levels of any inflammatory marker.
Increased intake of fiber from fruits was associated with healthier levels of the inflammatory marker sCD163.
With respect to cardiovascular disease:
Every 5g/day increase in total fiber decreased the risk of heart disease by 5%.
Every 5g/day increase in fiber from whole grains decreased the risk of heart disease by 14%.
Increased intake of fiber from vegetables and fruits did not have a statistically significant effect on the risk of heart disease.
Finally, when the investigators did a statistical analysis to determine to extent to which the effect of whole grain fiber on inflammation, could explain its effect on heart disease, they concluded:
The effect of whole grain fiber on inflammation could explain only about 16% of its effect on heart disease.
In the words of the authors, “In this prospective study of older adults, higher intakes of total fiber were associated with lower levels of various inflammatory markers, and this inverse association was primarily due to cereal fiber intake. Vegetable and fruit fiber intakes were not consistently associated with lower levels of inflammatory markers. These results suggest that specifically cereal fibers might be more effective in reducing systemic infection, which will need to be tested in interventional studies of specific populations.
In addition, cereal fiber was associated with a lower risk of CVD, although inflammation mediated less than 20% of the observed inverse association between cereal fiber and CVD. This suggests that the association of cereal fiber is primarily due to factors … other than systemic inflammation.”
Note: This conclusion underplays the role of fruit fiber in reducing inflammation. The statement is correct in saying only whole grain fiber reduces the inflammatory markers CRP, IL-6, and IL-1RA. However, both total fiber and fruit fiber increase the anti-inflammatory marker sCD163. That is why I chose to use the term “healthier levels” rather than lower or higher levels when describing the effects of whole grain and fruit fibers on markers of inflammation.
What Does This Study Mean For You?
#1: The biggest takeaway from this study is that whole grains are good for you.
This study shows that whole grain fiber decreases our risk of developing heart disease.
This is fully consistent with multiple previous studies showing that whole grains decrease the risk of heart disease.
Previous studies have also shown that whole grains reduce the risk of cancer and diabetes.
This study also suggests that whole grain fiber reduces chronic inflammation.
There are also some takeaways from this and previous studies that may not be so obvious.
#2: Fiber has many important benefits beyond its effect on inflammation. For example:
This study concluded that the reduction in inflammation only explained a small part of the beneficial effect of whole grain fiber on reducing heart disease risk.
That is because whole grain fiber also:
Feeds friendly bacteria that improve gut function.
Provides satiety that can result in reduced fat and calorie intake.
Binds cholesterol, which improves blood cholesterol level.
Slows the rate at which dietary sugar enters the bloodstream, which improves blood sugar control.
#3: Whole plant foods have many benefits beyond their fiber content.
This study concluded that whole grain fiber was more beneficial than fiber from fruits and vegetables at reducing inflammation and reducing the risk of heart disease.
However, we know that fresh fruits and vegetables are an essential part of an anti-inflammatory diet.
Previous studies have also shown that fruit and vegetables significantly decrease the risk of heart disease, stroke, and cancer.
That is because whole grains and unprocessed fruits and vegetables:
Displace sugar, refined flour, and highly processed foods from the diet.
Have a lower caloric density than processed foods, making it easier to achieve a healthy weight.
Provide nutrients and phytonutrients not found in processed foods.
Support a wide variety of healthy gut bacteria.
Are Low Carb Diets Healthy Long Term?
When you consider all the benefits of whole grains, fresh fruits, and vegetables, it brings us to the final take home message.
#4: Despite what Dr. Strangelove has told you, low-carb diets may not be healthy long term.
There are no long-term (10 or 20-year) studies of low-carb diets. We simply have no evidence to support the claim that they are healthy long term.
Most low-carb diets eliminate or severely limit fruits and whole grains. Considering the many health benefits they provide, it is unlikely that any diet that restricts them is healthy long term.
The Bottom Line
A recent study looked at the effect of plant fiber on inflammation and on heart disease.
With respect to inflammation the study found:
Increased intake of total fiber was associated with healthier levels of the inflammatory markers CRP, IL-1RA, and sCD163.
Increased intake of fiber from whole grains was associated with healthier levels of the inflammatory markers CRP, IL-6, and IL-1RA.
Increased intake of vegetable fiber was not significantly associated with healthier levels of any inflammatory marker.
Increased intake of fiber from fruits was associated with healthier levels of the inflammatory marker sCD163.
With respect to cardiovascular disease:
Every 5g/day increase in total fiber decreased the risk of heart disease by 5%.
Every 5g/day increase in fiber from whole grains decreased the risk of heart disease by 14%.
The biggest takeaway from this study is that whole grains are good for you.
Other takeaways from this and previous studies are:
2) Fiber has many important benefits beyond its effect on inflammation.
3) Whole plant foods have many benefits beyond their fiber content.
4) Despite what Dr. Strangelove has told you, low-carb diets may not be healthy long term.
For more details on this study and what it means for you, read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure or prevent any disease.
If you believe the headlines, olive oil is a superfood. It is often described as the star of the Mediterranean diet. It is referred to as the healthiest of dietary fats. Is this true, or is it hype?
Olive oil’s resume is impressive:
It is rich in monounsaturated fatty acids, which…
Are less susceptible to oxidation than polyunsaturated oils.
Make our arteries more flexible, which lowers blood pressure.
Lower LDL-cholesterol levels, which reduces the risk of heart disease.
Extra-virgin olive oil contains phytonutrients and tocopherols (various forms of vitamin E), which…
Have anti-inflammatory properties.
Improve insulin sensitivity and blood sugar control.
Olive oil consumption is also associated with healthier gut bacteria, but it is not clear whether this is due to olive oil or to the fact that a Mediterranean diet is also richer in fresh fruits, vegetables, and whole grains.
Several recent studies have shown that olive oil consumption is associated with a lower risk of heart disease. However, these studies were conducted in Mediterranean countries where the average intake of olive oil (3 tablespoons/day) is much greater than in the United States (0.3 tablespoons/day).
The amount of olive oil Americans consume decreases the risk of heart disease.
Whether olive oil consumption had benefits beyond a reduction in heart disease risk.
How Was This Study Done?
This study combined data from 60,582 women enrolled in the Nurses’ Health Study and 31,801 men enrolled in the Health Professionals Follow-Up Study). The participants:
Were free of heart disease and diabetes at the start of the study.
Were 56 at the start of the study with an average BMI of 25.6 (Individuals with BMIs in the 25-30 range are considered overweight, so they were at the lowest end of the overweight range).
The Nurses’ Health Study and Health Professional Follow-Up Study are both association studies, meaning they looked at the association between olive oil consumption and health outcomes. They cannot directly prove cause and effect. However, they are very strong association studies because:
Every 2 years, participants filled out a questionnaire that updated information on their body weight, smoking status, physical activity, medications, multivitamin use, and physician-diagnosed diseases.
Every 4 years, participants filled out a comprehensive food frequency questionnaire.
In other words, this study did not just rely on the participant’s lifestyle, dietary intake, and health at the beginning of the study, as so many association studies do. It tracked how each of these variables changed over time.
The participants were followed for an average of 28 years and their average olive oil intake over those 28 years was correlated with all-cause mortality and mortality due to specific diseases.
Deaths were identified from state vital statistics, the National Death index, reports by next of kin, or reports by postal authorities.
Causes of death were determined by physician review of medical records, medical reports, autopsy reports, or death certificates.
Does Olive Oil Help You Live Longer?
During the 28 years of this study:
Olive oil consumption in the United States increased from an average of ~1/3 teaspoon/day to ~1/3 tablespoon/day.
Margarine consumption decreased from 12 g/day to ~4 g/day.
The consumption of all other fats and oils remained about the same.
As I mentioned above, olive oil consumption was averaged over the life of the study for each individual. When the investigators compared people consuming the highest amount of olive oil (>0.5 tablespoon/day) with people consuming the least olive oil (0 to 1 teaspoon/day):
Mortality from all causes was decreased by 35% for the group consuming the most olive oil.
However, the group consuming the most olive oil also was more physically active, had a healthier diet, and consumed more fruits and vegetables than the group who consumed the least olive oil.
After correcting for all those factors, mortality from all causes was decreased by 19% for the group consuming the most olive oil.
The authors concluded, “We found that greater consumption of olive oil was associated with lower risk of total…mortality… Our results support current dietary recommendations to increase the intake of olive oil…to improve overall health and longevity.” (I will fill in the blanks in this statement once I have covered other aspects of this study)
The authors also said, “Of note, our study showed that benefits of olive oil can be observed even when consumed in lower amounts than in Mediterranean countries.”
Are There Other Benefits From Olive Oil Consumption?
The study didn’t stop there. The investigators also looked at the effect of olive oil consumption on the major killer diseases in the United States and other developed countries. When they compared the effect of olive oil consumption on cause-specific mortality, they found that the group who consumed the most olive oil reduced their risk of dying from:
Cardiovascular disease by 19%.
Cancer by 17%
Respiratory disease by 18%.
Neurodegenerative disease (cognitive decline and Alzheimer’s disease) by 29%.
The reduction in neurodegenerative disease was much greater for women (34% decrease) than for men (19% decrease).
With this information I can fill in one of the blanks in the author’s conclusions: “We found that greater consumption of olive oil was associated with lower risk of total and cause-specific mortality… Our results support current dietary recommendations to increase the intake of olive oil…to improve overall health and longevity.”
Which Fats Are Healthiest?
The sample size was large enough and the dietary information complete enough for the investigators to also estimate the effect of substituting olive oil for other dietary fats and oils.
They found that every ¾ tablespoon of olive oil substituted for an equivalent amount of:
Margarine decreased total mortality by 13%.
Butter decreased total mortality by 14%.
Mayonnaise deceased total mortality by 19%
Dairy fat decreased total mortality by 13%.
The same beneficial effects of substituting olive oil for other fats were seen for cause-specific mortality (cardiovascular disease, cancer, respiratory disease, and neurodegenerative disease).
There was a linear dose-response. This means that substituting twice as much olive oil for other dietary fats doubled the beneficial effects on total and cause-specific mortality.
However, substituting olive oil for polyunsaturated vegetable oils had no effect on total and cause-specific mortality.
Now I can fill in the remaining blanks in the author’s conclusion: “We found that greater consumption of olive oil was associated with lower risk of total and cause-specific mortality. Replacing other types of fat, such as margarine, butter, mayonnaise, and dairy fat, with olive oil was also associated with a lower risk of mortality. Our results support current dietary recommendations to increase the intake of olive oil and other unsaturated vegetable oils in place of other fats to improve overall health and longevity.”
What Does This Study Mean For Us?
As I said above, this is an association study, and association studies do not prove cause and effect. However:
1) This is a very strong association study because:
It is a very large study (92,383 participants).
It followed the participants over a long time (28 years).
It utilized a very precise dietary analysis.
Most importantly, it tracked the participant’s lifestyle, dietary intake, and health at regular intervals throughout the study. Most association studies only measure these variables at the beginning of the study. They have no idea how they change over time.
2) This study is consistent with several previous studies showing that olive oil consumption decreases the risk of dying from heart disease.
3) This study draws on its large population size and precise dietary analysis to strengthen and extend the previous studies. For example:
The study showed that increased olive oil consumption also reduced total mortality and mortality due to cancer, respiratory disease, and neurodegenerative disease.
The study measured the effect of substituting olive oil for other common dietary fats.
The study showed that increased olive oil consumption in the context of the American diet was beneficial.
I should point out that the headlines you have seen about this study may be misleading.
While the headlines may have depicted olive oil as a superfood, this study did not find evidence that olive oil was more beneficial than other unsaturated vegetable oils. Again, this is consistent with many previous studies showing that substituting vegetable oils for other dietary fats reduces the risk of multiple diseases.
The headlines focused on the benefits of increasing olive oil consumption. However, they neglected the data showing that increasing olive oil (and other vegetable oils) was even more beneficial (35% reduction in total mortality) in the context of a healthy diet – one with increased intake of fruits, vegetables, whole grains, nuts, legumes, and long-chain omega-3s and decreased intake of red & processed meats, sodium, and trans fats.
So, my recommendation is to follow a whole food, primarily plant-based diet and substitute extra-virgin olive oil and cold pressed vegetable oils for some of the animal fats in your diet.
Some vegan enthusiasts recommend a very low-fat whole food plant-based diet. They point to studies showing that such diets can actually reverse atherosclerosis. However:
Those studies are very small.
The overall diet used in those studies is a very healthy plant-based diet.
The studies did not include a control group following the same diet with olive oil or other vegetable oils added to it, so there is no comparison of a healthy vegan diet with and without vegetable oils.
If you have read my book, “Slaying the Food Myths”, you know that my recommendations encompass a variety of whole food, primarily plant-based diets ranging all the way from very-low fat vegan diets to Mediterranean and DASH diets. Choose the one that best fits your food preferences and the one you will be most able to stick with long term. You will be healthier, and you may live longer.
The Bottom Line
A recent study looked at the effect of olive oil consumption on the risk dying from all causes and from heart disease, cancer, respiratory disease, and neurodegenerative diseases. When the study compared people consuming the highest amount of olive oil (>0.5 tablespoon/day) with people consuming the least olive oil (0 to 1 teaspoon/day):
Mortality from all causes was decreased by 19% for the group consuming the most olive oil.
They also found that the group who consumed the most olive oil reduced their risk of dying from:
Cardiovascular disease by 19%.
Cancer by 17%
Respiratory disease by 18%.
Neurodegenerative disease (cognitive decline and Alzheimer’s disease) by 29%.
They also found that every ¾ tablespoon of olive oil substituted for an equivalent amount of:
Margarine decreased total mortality by 13%.
Butter decreased total mortality by 14%.
Mayonnaise deceased total mortality by 19%
Dairy fat decreased total mortality by 13%.
However, substituting olive oil for polyunsaturated vegetable oils had no effect on total and cause-specific mortality.
The authors concluded, “We found that greater consumption of olive oil was associated with lower risk of total and cause-specific mortality. Replacing other types of fat, such as margarine, butter, mayonnaise, and dairy fat, with olive oil was also associated with a lower risk of mortality. Our results support current dietary recommendations to increase the intake of olive oil and other unsaturated vegetable oils in place of other fats to improve overall health and longevity.”
For more details and a summary of what this study means for you, read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure or prevent any disease.
I was pondering what to write about in this month’s newsletter and then I had three clients come in, all suffering from the same problem. That made up my mind. The topic this month is thumb pain.
Several years ago, when I was still in New York, I had a regular client come in and tell me she had just been told she had arthritis in her thumb joint. I asked how she knew that, and she showed me her hand. Her thumb was bent all the way in toward her palm and when she tried to bring her hand flat, the joint was painful, preventing her thumb from moving.
She had been given medications for the arthritis, but when she checked it out on the internet, the potential side-effects scared her so much she decided to just suffer with the arthritis.
But it wasn’t arthritis at all. The pain she was experiencing was caused by a tight muscle. I taught her the self-treatment I’m going to show you, and the results were fantastic!
Why a Tight Muscle Causes the Symptoms of Arthritis of the Thumb Joint
We use our thumbs uncountable times every day. It is impossible to even consider how many times we have used our thumb muscles over the course of our lives, but we never think about the muscles that enable us to do that movement. Yet, think of what life would be like if you lost your ability to use your thumb.
Your thumb muscle, called Opponens Pollicis, originates on the ligament that forms the bridge to your carpal tunnel. (More about carpal tunnel syndrome in a future newsletter) It inserts into the joint that is at the base of your thumb. It forms the bulge at the base of your thumb, right where the thumb of the right hand, shown on the graphic on the left, is pressing into the left hand.
For example, do the movement shown above, pressing your right thumb into the thick muscle at the base of your thumb. Then move your left thumb in toward the palm of your hand. You’ll feel the muscle contract.
As the muscle is repetitively strained it shortens. The problem is, as it’s shortening it is pulling on the bridge to the carpal tunnel and moving your thumb in toward your palm. When it gets tight, if you try to bring your thumb out it will pull at the joint. It’s like pulling your hair and then your scalp hurts.
The good news is it’s simple to release the tension in the muscle fibers, it just takes a long time to get it to fully release.
Treatment For A Painful Thumb
It’s simple to treat your Opponens Pollicis muscle.
Place your opposite elbow directly onto the muscle. Wrap your fingers around your elbow to stabilize it so it won’t slide off the muscle.
Press deeply into the muscle and either stay still or move very slightly back and forth to lengthen the muscle fibers.
Or you can…
Place your bent middle finger directly into the muscle and wrap your hand around your hand to stabilize so your knuckle won’t keep sliding off the muscle.
Hold the pressure for about 30 seconds and then move ¼” along them muscle to a new spot.
I developed this technique when I had carpal tunnel syndrome. It took me hours of self-treatment to get the muscle to final relax and not be painful. That’s when you know you have finally released the tension and the strain is removed from the bridge to your carpal tunnel (flexor retinaculum).
Even if you don’t have the symptoms of carpal tunnel syndrome, doing this technique will make your hand feel so much better, more flexible, and light.
Treat Yourself to Pain-Free Living!
It’s the name of my book, and it says exactly what you will experience when you discover how to release tight muscles that cause joint pain.
People have told me this book is their first “go to” when they have aches and pains, and it has saved them hundreds of dollars in doctor visits and pain medications.
For only $49.00 you can treat muscles that cause everything from headaches to foot pain…a bargain at twice the price!
Order Now and start to feel more flexible and pain-free quickly.
Wishing you well,
Julie Donnelly
www.FlexibleAthlete.com
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure, or prevent any disease.
Most of us look forward to our golden years – that mystical time when we will be free from the workday pressures and have more time to spend with friends and family doing the things we love.
But cognitive decline can cast a dark cloud over those expectations.
By the age of 65, 11% of adults suffer from some degree of cognitive impairment.
And by the age of 80 the percentage of adults suffering from cognitive impairment has increased to 26-30%, depending on which study you cite.
The results of cognitive decline can be devastating.
First you start to lose the cherished memories of a lifetime.
Then comes confusion and an inability to perform basic tasks and participate in your favorite activities.
Eventually you may reach a stage where you no longer recognize the ones you love.
In short, cognitive decline can rob you of everything that makes you you.
The causes of cognitive decline are complex, but recent studies have pointed to the role of chronic inflammation in cognitive decline. If that is true, it is a good news – bad news situation.
The bad news is:
Some increase in chronic inflammation appears to be an inevitable consequence of aging.
Chronic inflammation can be caused by certain diseases that are beyond our control.
Chronic inflammation can be triggered by viral or bacterial infections.
The good news is that chronic inflammation is also controlled by your diet and lifestyle. For example, as I said above, chronic inflammation is often triggered by a viral infection, but whether the inflammation is mild or severe is strongly influenced by diet and lifestyle.
The data for this study were taken from the first three years of the Hellenic Longitudinal Investigation of Aging and Diet (HELIAD), a study designed to look at the effect of diet on dementia and other neuropsychiatric conditions in the Greek population.
There were 1059 participants (40% male, average age = 75 at the beginning of the study) in this study. At the beginning of the study the participants completed a food frequency questionnaire administered by a trained dietitian. The foods were broken down into individual nutrients using the USDA Food Composition tables adapted for foods in the Greek diet.
The diet of each participant was then rated on a 15-point scale ranging from pro-inflammatory to anti-inflammatory based on something called the Diet Inflammation Index (DII).
Simply put, the DII is a validated assessment tool based on the effect of food nutrients on 6 inflammatory biomarkers found in the blood (IL-1β, IL-4, IL-6, IL-10, TNF-α, and CRP). Nutrients that decrease these markers are considered anti-inflammatory. Nutrients that increase these inflammatory biomarkers are considered pro-inflammatory.
For example, anti-inflammatory nutrients include:
Carotenoids and flavonoids (found in fruits and vegetables).
Omega-3 polyunsaturated fatty acids (found in cold-water fish, walnuts, flaxseeds, and chia seeds).
Monounsaturated fatty acids (found in olive, avocado, and peanut oils).
Fiber (found in minimally processed plant foods).
Antioxidants, most B vitamins, and vitamin D.
Magnesium and zinc.
Garlic, onions, most herbs & spices.
Pro-inflammatory nutrients include:
Refined carbohydrates.
Cholesterol.
Total fat.
Saturated fats.
Trans fats.
The participants were followed for 3 years, and all new diagnoses of dementia were recorded. The diagnoses were confirmed by a panel of neurologists and neuropsychologists.
Can Your Diet Cause You To Lose Your Mind?
As described above, the diet of each participant in the study was rated on a 15-point DII (Diet Inflammatory Index) scale ranging from pro-inflammatory to anti-inflammatory. The association of the DII score of the participant’s diets with the onset of dementia was evaluated in two ways.
Each one-point increase from an anti-inflammatory diet to a pro-inflammatory diet was associated with a 21% increase in the risk for dementia.
In other words, even small changes in your diet can have a significant impact on your risk of developing dementia.
The investigators then divided the participants into three equal-sized groups based on the DII score of their diets.
The group with the highest DII scores were 3 times more likely to develop dementia than the group with the lowest DII scores.
In other words, a major change in your diet can have a major effect on your risk of developing dementia.
The authors concluded, “In the present study, higher DII scores (indicating greater pro-inflammatory diet potential) were associated with an increased risk for incident dementia [newly diagnosed dementia]. These findings may avail the development of primary dementia strategies through tailored and precise dietary interventions.”
What Is A Mind-Healthy Diet?
This and other studies show that an anti-inflammatory diet is good for the mind. It helps protect us from cognitive decline and dementia. But what does an anti-inflammatory diet look like?
One hint comes from analyzing the diets of participants in this study:
Those with the lowest DII scores (most-anti-inflammatory diets) consumed 20 servings of fruit, 19 servings of vegetables, 4 servings of beans or other legumes, and 11 servings of coffee or tea each week. That’s almost 3 servings of fruit and 3 servings of vegetables every day!
Those with the highest DII scores (most pro-inflammatory diets) consumed only half as many fruits, vegetables, and legumes.
In short, a diet rich in fruits, vegetables, and legumes is a good start.
I have described anti-inflammatory diets in more detail in a previous issue of “Health Tips From the Professor.” Let me summarize that article briefly.
Anti-inflammatory foods include:
Colorful fruits and vegetables.
Whole grains.
Beans and other legumes.
Nuts, olive oil, avocados, and other sources of monounsaturated fats.
Fatty fish and other sources of omega-3 fatty acids.
Herbs and spices.
Pro-inflammatory foods include:
Refined carbohydrates, sodas, and sugary foods.
Foods high in saturated fats including fatty and processed meats, butter, and high fat dairy products.
Foods high in trans fats.
French fries, fried chicken, and other fried foods.
Foods you are allergic or sensitive food. For example, gluten containing foods are pro-inflammatory only if you are sensitive to gluten.
If your goal is to reduce chronic inflammation and keep your mind sharp as a tack as you age, you should eat more anti-inflammatory foods and less pro-inflammatory foods.
Of course, we don’t just eat random foods, we follow dietary patterns. It should be apparent from what I have covered above that whole food, primarily plant-based diets are anti-inflammatory. This is true for diets ranging from vegan through semi-vegetarian, to the Mediterranean, DASH, and MIND diets.
All these diets are anti-inflammatory and likely protect the brain from cognitive decline. However, the best evidence for brain protection is for the Mediterranean, DASH, and MIND diets.
The Mediterranean and DASH diets have been shown to prevent cognitive decline in multiple studies.
The MIND diet is a combination the Mediterranean and DASH diets that was specifically designed to prevent cognitive decline. It has been shown to cut the risk of developing Alzheimer’s disease in half.
What Is A Mind-Healthy Lifestyle?
Diet is just one aspect of a holistic approach for reducing cognitive decline as we age. Other important factors include:
Reduce excess body weight.
Exercise regularly.
Get adequate sleep.
Reduce and/or manage stress.
Eliminate smoking and reduce alcohol consumption.
Socialize with friends and family who support you. Numerous studies have shown that a strong support network reduces dementia risk in the elderly.
Keep your brain active. Work crossword puzzles. Learn new things. An active brain is forced to lay down new neural pathways.
The Bottom Line
Recent studies have suggested that chronic inflammation increases the risk of cognitive decline and dementia as we age. Some causes of chronic inflammation are beyond our control, but others, such as diet, we can control.
Recently, a precise scoring system called the Diet Inflammatory Index (DII) has been developed. This scoring system allows studies to look at the correlation between the inflammatory potential of the diet and cognitive decline.
A recent study enrolled 1,000 participants with an average age of 75 in a 3-year study to determine the impact of diet on cognitive decline. The association of the DII score of the participant’s diets with the onset of dementia was evaluated in two ways.
Each one-point increase from an anti-inflammatory diet to a pro-inflammatory diet was associated with a 21% increase in the risk for dementia.
In other words, even small changes in your diet can have a significant impact on your risk of developing dementia.
The investigators then divided the participants into three equal-sized groups based on the DII score of their diets.
The group with the highest DII scores were 3 times more likely to develop dementia than the group with the lowest DII scores.
In other words, a major change in your diet can have a major effect on your risk of developing dementia.
The authors concluded, “In the present study, higher DII scores (indicating greater pro-inflammatory diet potential) were associated with an increased risk for incident dementia [newly diagnosed dementia]. These findings may avail the development of primary dementia strategies through tailored and precise dietary interventions.”
For more details and a description of mind-healthy diets and a mind-healthy lifestyle read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure or prevent any disease.
 Omega-3s have become the latest “super food”. Wherever you get your news, you are constantly seeing articles about the latest “miracle results” obtained by adding omega-3s to your diet.
Omega-3s have become the latest “super food”. Wherever you get your news, you are constantly seeing articles about the latest “miracle results” obtained by adding omega-3s to your diet. The authors of this study enrolled 40 obese (BMI≥30) adults (40% females, 60% males), aged 30-50 in a randomized, active placebo-controlled, double-blind weight loss study for 8 weeks.
The authors of this study enrolled 40 obese (BMI≥30) adults (40% females, 60% males), aged 30-50 in a randomized, active placebo-controlled, double-blind weight loss study for 8 weeks. Because both groups had equal caloric restriction. Therefore, as expected, both groups experienced decreased:
Because both groups had equal caloric restriction. Therefore, as expected, both groups experienced decreased: The study also found that:
The study also found that: This study is a randomized, double-blind, placebo-controlled trial, which is the gold standard for clinical studies. But it is also a very small study, so we need to carefully consider the validity of the study.
This study is a randomized, double-blind, placebo-controlled trial, which is the gold standard for clinical studies. But it is also a very small study, so we need to carefully consider the validity of the study. Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years.
Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years.