Is It Meat Or Something Else?
Author: Dr. Stephen Chaney
 We are told we should be consuming more protein. But where should we get our protein?
We are told we should be consuming more protein. But where should we get our protein?
Meat is an obvious choice. But meat consumption is controversial. The arguments are intense.
There are those who claim that meat consumption, particularly red meat, increases our risk of cancer, heart disease, diabetes, and many other diseases. Others claim that meat has been maligned. It doesn’t increase disease risk. We should eat more of it, not less.
The problem is that both sides are basing their claims on published clinical studies. Studies on meat consumption and disease risk are all over the map.
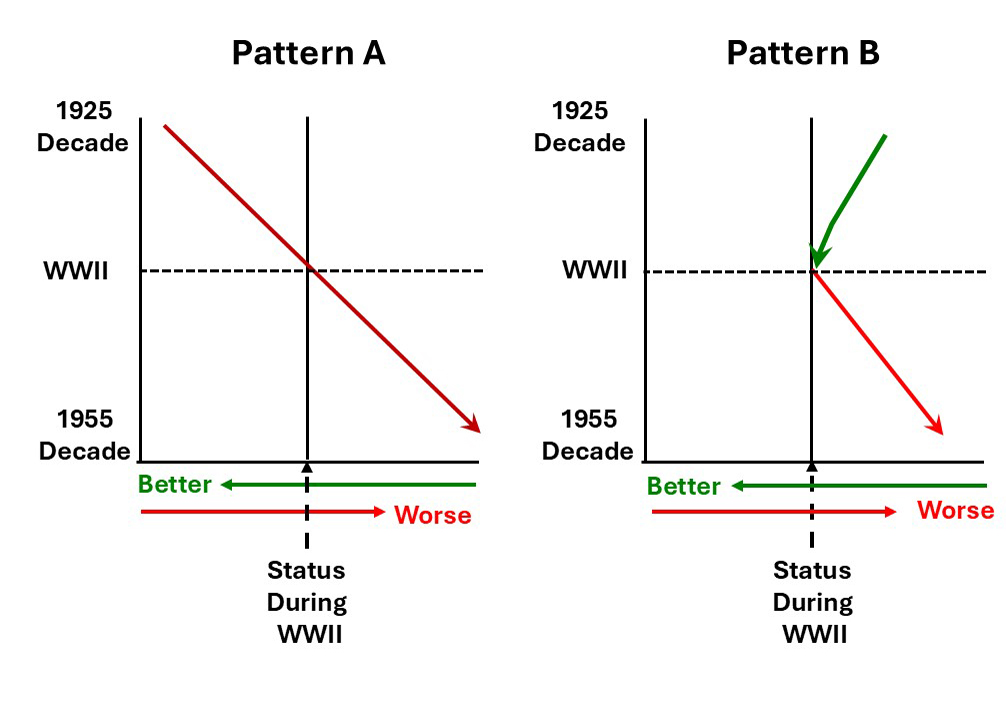
I have covered this controversy in previous issues of “Health Tips From the Professor”. In attempting to make sense of the conflicting data I made the observation that studies showing meat consumption reduced disease risk tended to come from third world countries while studies showing meat consumption increased disease risk tended to come from high-income western countries.
So, my interest was peaked when I saw a very large study (K Papier et al, BMC Medicine,: 19:53, 2021) on meat consumption and disease risk in the UK.
How Was This Study Done?
 The investigators used data from the UK Biobank Study, a study that recruited 503,317 young men and women throughout the UK between 2006 and 2010. Upon entry into the study participants completed questionnaires about physical data (height, weight, etc), biological data (blood sugar, cholesterol levels, etc.), and diet.
The investigators used data from the UK Biobank Study, a study that recruited 503,317 young men and women throughout the UK between 2006 and 2010. Upon entry into the study participants completed questionnaires about physical data (height, weight, etc), biological data (blood sugar, cholesterol levels, etc.), and diet.
This particular study used data from a subset (474,985) participants who completed a 24-hour dietary recall questionnaire.
Participants were then linked to the National Health Service database to assess the first occurrence of the 25 leading non-cancerous causes of hospital admissions for each patient and followed for an average of 8 years.
Cancer admissions were excluded from this study because the International Agency for Research on Cancer (IARC), the cancer agency of the WHO, has already classified red meat as a probable carcinogen and processed meat as a likely carcinogen.
Does Meat Consumption Increase Disease Risk?
 The investigators looked at four distinct categories of meat consumption (total meat, red meat, processed meat, and poultry) and the risk of 25 common diseases (excluding cancer). In each case, they divided meat consumption into quartiles and compared the disease risk for those in the highest quartile to those in the lowest quartile.
The investigators looked at four distinct categories of meat consumption (total meat, red meat, processed meat, and poultry) and the risk of 25 common diseases (excluding cancer). In each case, they divided meat consumption into quartiles and compared the disease risk for those in the highest quartile to those in the lowest quartile.
For the sake of simplicity, I will only report the most significant disease risks (those with p ≤001).
Total Meat Consumption (Lowest quartile = 1.2 oz/d; Highest quartile = 4.1 oz/d):
| Disease | Increased
Risk |
| Heart Disease | 29% |
| Stroke | 24% |
| Diverticular Disease | 29% |
| Colon Polyps | 14% |
| Diabetes | 85% |
Red Meat Consumption (Lowest quartile = 0.2 oz/d; Highest quartile = 2.0 oz/d):
| Disease | Increased
Risk |
| Heart Disease | 25% |
| Stroke | NS |
| Diverticular Disease | 26% |
| Colon Polyps | 11% |
| Diabetes | 53% |
Processed Meat Consumption (Lowest quartile = 0.15 oz/d; Highest quartile = 1.0 oz/d):
| Disease | Increased
Risk |
| Heart Disease | 17% |
| Stroke | 23% |
| Diverticular Disease | 18% |
| Colon Polyps | 11% |
| Diabetes | 52% |
Poultry Consumption (Lowest quartile = 1.2 oz/d; Highest quartile = 4.1 oz/d):
| Disease | Increased
Risk |
| Heart Disease | 12% |
| Stroke | NS |
| Diverticular Disease | 18% |
| Colon Polyps | 11% |
| Diabetes | 32% |
| GERD | 16% |
| Gastritis | 10% |
My evaluation of the data is:
- These differences are highly significant (p <001) and the study size was very large (~475,000 participants), so the increased risk is probably true for a high-income Western country like the UK.
-
- However, some of these differences are relatively small. It’s easy to understand how they might be missed in smaller studies.
-
- Even increased risk in the 25-30% range might disappear in studies that combine data from high-income countries and third world countries.
-
- With this perspective it is easy to understand why previous studies have been so confusing.
- Because the investigators looked at the effect of each kind of meat separately, one can get a better idea of the relative contribution of each meat to various diseases [With, of course, the caveat that people who consume more red meat also tend to consume more processed meat and vice versa.] For example:
-
- Red meat appears to contribute more to heart disease risk than processed meat or poultry – possibly due to its high saturated fat and cholesterol content.
-
- Processed meat appears to contribute more to stroke risk than red meat or poultry – possibly due to added nitrates and other food additives.
-
- All meats appear to contribute to diverticular disease – possibly due to a change in gut bacteria because meats replace plant foods in the diet.
- The increased risk of GERD and gastritis associated with poultry consumption was surprising, but the increased risk was small.
The authors concluded, “Our findings from this large prospective study of British adults show that meat consumption is associated with higher risks of several common conditions but a lower risk of iron deficiency anemia…Additional research is needed to evaluate whether these differences in risk reflect causal relationships, and if so what proportion [of these outcomes] could be prevented by decreasing meat consumption.”
Is It Meat Or Something Else?
 Of course, the question, “Is it meat or something else in our diet that is causing the increased risk of disease?” One hint that something else might be contributing to disease risk came when the authors corrected the data for obesity. The results are shown below:
Of course, the question, “Is it meat or something else in our diet that is causing the increased risk of disease?” One hint that something else might be contributing to disease risk came when the authors corrected the data for obesity. The results are shown below:
Total Meat Consumption Corrected For Obesity
| Disease | Increased
Risk |
Corrected
For Obesity |
| Heart Disease | 29% | 17% |
| Stroke | 24% | 22% |
| Diverticular Disease | 29% | 18% |
| Colon Polyps | 14% | 10% |
| Diabetes | 85% | 33% |
Red Meat Consumption Corrected For Obesity
| Disease | Increased
Risk |
Corrected
For Obesity |
| Heart Disease | 25% | 16% |
| Stroke | NS | NS |
| Diverticular Disease | 26% | 17% |
| Colon Polyps | 11% | 8% |
| Diabetes | 53% | 21% |
Processed Meat Consumption Corrected For Obesity
| Disease | Increased
Risk |
Corrected
For Obesity |
| Heart Disease | 17% | 9% |
| Stroke | 23% | 17% |
| Diverticular Disease | 18% | 17% |
| Colon Polyps | 11% | 8% |
| Diabetes | 52% | 24% |
Poultry Consumption Corrected For Obesity
| Disease | Increased
Risk |
Corrected
For Obesity |
| Heart Disease | 12% | 8% |
| Stroke | NS | NS |
| Diverticular Disease | 14% | 10% |
| Colon Polyps | 6% | 7% |
| Diabetes | 32% | 14% |
| GERD | 16% | 17% |
| Gastritis | 10% | 12% |
When corrected for obesity, the risk of:
- Heart disease decreased by 33-47%.
- Diverticular disease decreased by 23-38%.
- Diabetes decreased by 54-61%.
But how do we interpret that? It would be easy to conclude that the influence of meat consumption on heart disease, diverticular disease, and diabetes is small. However, that’s not the real world. People aren’t meat eaters or overweight. In the real world, people are often meat eaters and overweight.
So, the important question to ask is why so many meat eaters are overweight.
- It could simply be a question of calories. A serving of steak is around 680 calories, while a serving of beans is around 110 calories.
- It could be what is eaten with the steak or beans. A medium baked potato with butter and sour cream adds 300-500 calories. A vegetable stir fry adds 170 calories.
- It could be how we cook it. In our country over 50% of chicken we eat is fried. And to make matters worse, we often add French Fries and other highly processed foods to our fried chicken meal.
What Does This Study Mean For You?
 This study shows that in a high-income western society like ours, meat consumption is likely to increase our risk of several diseases, For example:
This study shows that in a high-income western society like ours, meat consumption is likely to increase our risk of several diseases, For example:
- Red meat is associated with increased risk of heart disease, diabetes, and diverticular disease.
- Processed meat is associated with increased risk of stroke, diabetes, and diverticular disease.
- Poultry consumption is associated with increased risk of diabetes and digestive diseases.
- All three kinds of meat are associated with obesity.
While it is easy to blame meat consumption for all our ills, it may be how we cook it and what we eat along with it.
Perhaps we should eat our meat the way they do in Third World countries. Rather than eating it as a main course, perhaps we should use it as flavoring for a vegetable stir fry or a lentil stew.
The Bottom Line
A recent study looked at the association of meat consumption with disease risk in the UK. It found that:
- Red meat is associated with increased risk of heart disease, diabetes, and diverticular disease.
- Processed meat is associated with increased risk of stroke, diabetes, and diverticular disease.
- Poultry consumption is associated with increased risk of diabetes and digestive diseases.
- All three kinds of meat are associated with obesity.
For more information on this study and what it means for you, read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure or prevent any disease.
____________________________________________________________________________
My posts and “Health Tips From the Professor” articles carefully avoid claims about any brand of supplement or manufacturer of supplements. However, I am often asked by representatives of supplement companies if they can share them with their customers.
My answer is, “Yes, as long as you share only the article without any additions or alterations. In particular, you should avoid adding any mention of your company or your company’s products. If you were to do that, you could be making what the FTC and FDA consider a “misleading health claim” that could result in legal action against you and the company you represent.
For more detail about FTC regulations for health claims, see this link.
https://www.ftc.gov/business-guidance/resources/health-products-compliance-guidance
______________________________________________________________________
About The Author
 Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years. Dr. Chaney won numerous teaching awards at UNC, including the Academy of Educators “Excellence in Teaching Lifetime Achievement Award”. Dr Chaney also ran an active cancer research program at UNC and published over 100 scientific articles and reviews in peer-reviewed scientific journals. In addition, he authored two chapters on nutrition in one of the leading Biochemistry textbooks for medical students.
Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years. Dr. Chaney won numerous teaching awards at UNC, including the Academy of Educators “Excellence in Teaching Lifetime Achievement Award”. Dr Chaney also ran an active cancer research program at UNC and published over 100 scientific articles and reviews in peer-reviewed scientific journals. In addition, he authored two chapters on nutrition in one of the leading Biochemistry textbooks for medical students.
Since retiring from the University of North Carolina, he has been writing a weekly health blog called “Health Tips From the Professor”. He has also written two best-selling books, “Slaying the Food Myths” and “Slaying the Supplement Myths”. And most recently he has created an online lifestyle change course, “Create Your Personal Health Zone”. For more information visit https://chaneyhealth.com.
For the past 54 years Dr. Chaney and his wife Suzanne have been helping people improve their health holistically through a combination of good diet, exercise, weight control and appropriate supplementation.