A Brief History Of USDA Food Guides
Author: Dr. Stephen Chaney
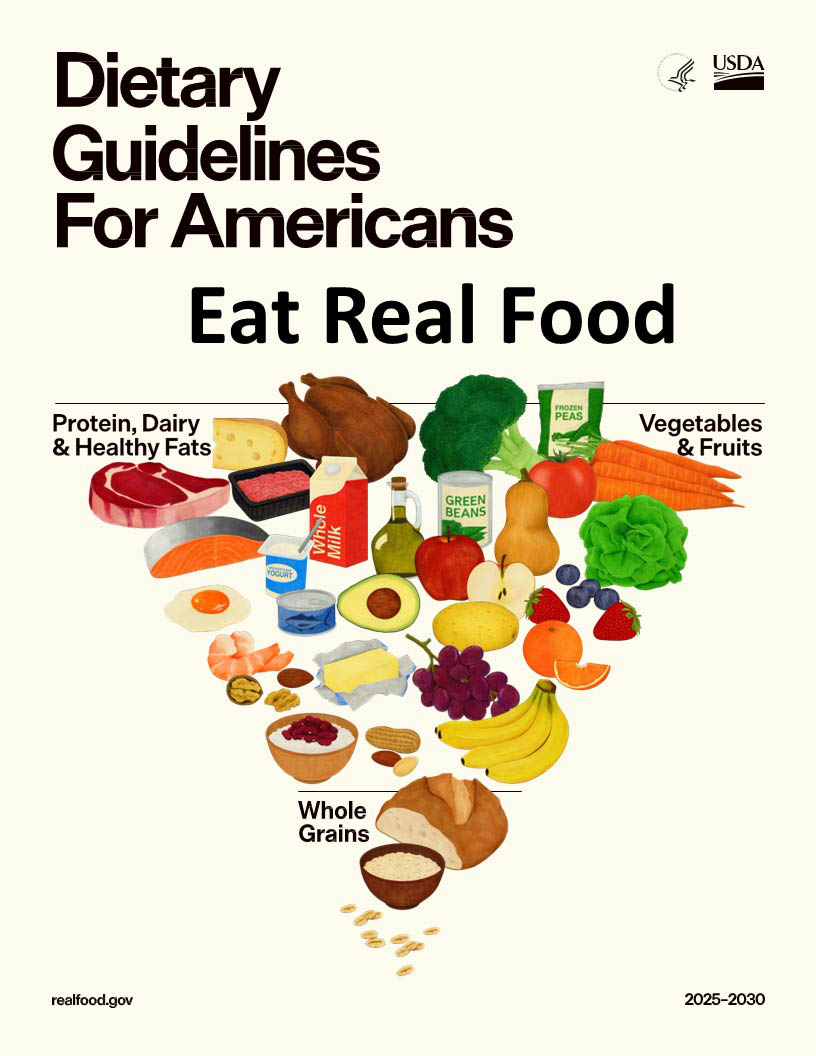 Unless you have cut yourself off from all outside media, you already know the USDA has just released new “Dietary Guidelines For Americans” and a new, upside down, food pyramid.
Unless you have cut yourself off from all outside media, you already know the USDA has just released new “Dietary Guidelines For Americans” and a new, upside down, food pyramid.
Both the AMA and AHA have endorsed the new guidelines with some reservations. But like everything else in today’s world they have become both political and controversial.
- Some experts are saying, “The new guidelines are fantastic. They will make Americans much healthier. It’s about time the government caught up with the latest scientific advances.
- Others are saying, “The new guidelines are terrible. They will set medicine back 20 years.”
As usual, the truth lies somewhere in the middle. I will explore that middle ground and discuss the pros and cons of the new dietary guidelines and food guide pyramid in this article.
But first we should start with something everyone can agree with, “What we are doing now isn’t working!” For example:
- The percentage of Americans who are overweight or obese is approaching 70%.
- The United States spends more on healthcare per person than any other country in the world. But we…
-
- Rank 48th in life expectancy. We not only rank below every developed country, but we also rank below many 3rd world countries.
-
-
- And we are losing ground. In 1990, we ranked 35th in life expectancy.
-
-
- Rank 69th in health span (healthy life expectancy).
-
-
- Again, we are losing ground. Our ranking was 42nd in 1990.
-
-
- Rank dead last (183rd out of 183) in health span as a percentage of life expectancy.
In short, we are falling behind the rest of the world in terms of lifespan, health span, and percentage of healthy years.
And our deteriorating health is costly.
90% of our health care spending is for preventable diseases
A Brief History Of USDA Food Guides
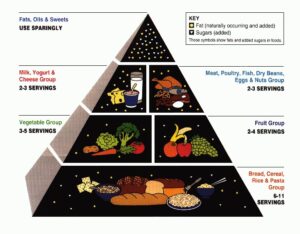 The USDA introduced the first food guide pyramid in 1992 based on the best nutrition science of the time. You probably remember the mantra:
The USDA introduced the first food guide pyramid in 1992 based on the best nutrition science of the time. You probably remember the mantra:
- 2-3 servings of dairy, preferably low fat.
- 2-3 servings in the protein category (lean meats, fish, dry beans, eggs, and nuts).
- 2-4 servings of fruits and 3-5 servings of vegetables.
- 6-11 servings of grains (bread, cereals, rice, and pasta).
- Fats, oils, and sweets were at the top of the pyramid with the caption, “Use Sparingly”.
This pyramid and the accompanying dietary guidelines were publicized so much that practically everyone knew them by heart.
Ten years later the USDA did a nutrition survey to see if their guidelines had changed American’s eating behavior. The answer was a clear, “No”. Only 5% of Americans ate according to the food guide pyramid.
The Geniuses at the USDA concluded that the food guide pyramid must be too difficult for the average American, so they introduced a simpler version, My Pyramid in 2005.
Guess what! Only 5% of Americans followed those recommendations, so they went to the super simple My Plate. By now you have probably guessed that only 5% of Americans followed the My Plate recommendations.
It turns out Americans weren’t confused by the recommendations. The recommendations were just too different from the way they were used to eating.
So, one change you will see in the new food guide pyramid is it includes some of Americans favorite foods, such as red meat, butter, and full fat dairy. Is that sacrilege or is it smart? Only time will tell.
With that in mind, let’s discuss the new “Dietary Guidelines For Americans”.
#1: Eat Real Food
 This is one recommendation that virtually everyone agrees with. The average American is getting 55% of their calories from highly processed foods. And the health consequences of that much processed food are devastating. Consumption of highly processed foods is linked to higher risk of:
This is one recommendation that virtually everyone agrees with. The average American is getting 55% of their calories from highly processed foods. And the health consequences of that much processed food are devastating. Consumption of highly processed foods is linked to higher risk of:
- Obesity.
- Type 2 diabetes.
- Heart attack.
- Stroke.
- Some cancers.
- Depression and anxiety.
- Dementia
- Premature death.
If you are wondering how we got to this point, the answer is simple. It stems from the desire of Americans to eat a healthier diet without giving up their favorite foods and the willingness of Big Food Inc (the food industry) to give us exactly what we want. For example:
- Some people want to eat a more plant-based diet, but don’t want to give up their favorite meats. Big Food Inc is only too happy to oblige. They mix some fat, salt, and a witch’s brew of chemicals to give us phony baloney, faken bacon, and everyone’s favorite, tofurkey.
- Some people are convinced keto diets are healthy, but don’t want to give their favorite sweets. Again, Big Food Inc is only too happy to oblige. They mix up a witch’s brew of chemicals to give us keto cookies and keto pastries.
I’m being facetious, but you get my point.
Some representatives of Big Food Inc claim that the health risks of processed foods are unproven. They are lying!
If you would like to read my reviews of major studies showing the health risks of highly processed foods, just go to https://www.chaneyhealth.com/healthtips/ and put “processed foods” in the search box.
#2: Prioritize Protein Foods at Every Meal
 This is one of the more controversial recommendations of the new food guide pyramid. The new USDA dietary guidelines increase the protein recommendation by 50-100% compared to previous versions…
This is one of the more controversial recommendations of the new food guide pyramid. The new USDA dietary guidelines increase the protein recommendation by 50-100% compared to previous versions…
- From 0.36 grams of protein per pound of body weight to…
- Between 0.54 and 0.72 grams of protein per pound of body weight.
[Note: If these numbers seem different from what you have seen, that is because the official recommendations are in grams of protein per kilogram of body weight. Since most Americans have no idea what their body weight is in kilograms, those numbers are useless.]
The main criticisms about the new protein recommendations are:
#1: “There isn’t solid evidence that most people need this much protein.”
My response is that anyone who makes that claim hasn’t kept up with the last two decades of protein research.
The old 0.36/pound standard is probably OK for the average middle-aged couch potato, but higher protein intakes are needed for people who are:
- Active, especially if they are trying to increase muscle mass, strength, or endurance.
- Over 50 and are trying to maintain muscle mass, strength, and mobility.
- Trying to lose weight without losing muscle, especially if they are using GLP-1 drugs.
- Trying to reduce the risk of type 2 diabetes and other chronic diseases.
In short, almost everyone except the couch potatoes will benefit from higher protein intakes. And, yes, the latest science shows that it is best to get at least 20 grams of protein with each meal.
You can find more information about the science behind increased protein recommendations by going to https://www.chaneyhealth.com/healthtips/ and putting “protein” in the search box.
 #2: “The new guidelines don’t steer people towards plant proteins”. This is a subtle distinction. The new USDA dietary guidelines include plant protein sources. But they do not recommend that they replace some of the animal proteins in the diet, as did previous versions. This allows people to choose between animal and plant proteins based on their preferences.
#2: “The new guidelines don’t steer people towards plant proteins”. This is a subtle distinction. The new USDA dietary guidelines include plant protein sources. But they do not recommend that they replace some of the animal proteins in the diet, as did previous versions. This allows people to choose between animal and plant proteins based on their preferences.
Those of you who have been following my “Health Tips From the Professor” blog know that I am an advocate of primarily plant-based diets. I am fully in the “replace some animal protein with vegetable protein” camp.
- But I acknowledge that is not the way most Americans eat. Perhaps it is time to make dietary recommendations that align more closely with the way people eat if we want to get above 5% acceptance.
- It would also be difficult to meet the new protein guidelines with plant protein alone unless you add commercially available plant protein supplements.
#3: “Higher protein intakes may be harmful for some people”. Recent research has shown that this concern is overblown for most Americans. However, there are some people who should probably check with their doctor before they increase their protein intake.
- People who have been diagnosed with kidney disease.
- People with genetic conditions or diseases that predispose to kidney disease. One example would be poorly controlled diabetes. [Note: I do not mean to imply that higher protein intake is likely to cause kidney disease in these situations. I included this category because people in these situations may have undiagnosed kidney disease.]
In most of these cases, you have probably been warned by your doctor to be careful about excess protein intake. But if you are uncertain about your risk for kidney disease, it never hurts to check with your doctor before increasing your protein intake.
What About Red Meat?
 The new dietary guidelines have been criticized for emphasizing red meat. That criticism is inaccurate. It’s a “tempest in a teapot”.
The new dietary guidelines have been criticized for emphasizing red meat. That criticism is inaccurate. It’s a “tempest in a teapot”.
In fact, red meat is pictured in both the original and the most recent versions of the food guide pyramid. And red meat is mentioned as one source of protein in both the original and the latest versions of dietary guidelines. It is given no special emphasis over other protein sources in either version of the dietary guidelines.
However, I would like to share my perspective on red meat.
- Diet context matters. As I have said in previous issues of “Health Tips From The Professor”, fruits, vegetables, whole grains, and beans are the antidotes to all the bad aspects of red meat.” And if you look at the new food guide pyramid, red meat and other proteins are in the same neighborhood as fruits and vegetables.
- Amount matters. Think of red meat as a garnish – for example, 2-3 ounces of red meat as part of a steak salad or stir fry with lots of veggies rather than an 8-ounce steak with fries.
#3: Consume Dairy
 The new dietary guidelines differ from previous versions in both the amount and kind of dairy foods consumed. For example:
The new dietary guidelines differ from previous versions in both the amount and kind of dairy foods consumed. For example:
- The old guidelines recommended 2-3 servings of dairy foods per day.
-
- The new guidelines recommend 3 servings per day as part of a 2,000-calorie dietary pattern.
-
- Since most Americans consume 3,600 to 3,800 calories per day that recommendation translates to at least 5 servings per day.
- The old guidelines recommended choosing low fat dairy foods.
-
- The new guidelines say, “When consuming dairy, include full-fat dairy with no added sugars.”
Since the full-fat dairy recommendation is the most controversial change, I will address it first.
Let me start by saying that I have been a traditionalist with respect to dairy foods. I have recommended low-fat dairy foods for years. But a good scientist must be willing to change their recommendations based on the latest research findings.
And new findings have clearly challenged our perspective on full-fat dairy foods. Several large, well-designed studies over the past decade have shown that full-fat dairy foods are just as healthy as low-fat dairy foods. I will make two comments about these studies.
- I suspect that the studies may be skewed because much of the data on full-fat dairy comes from countries where most of full-fat dairy foods are fermented – and we know that fermented dairy foods are very healthy.
-
- Admittedly, I have no data to back up my suspicion, but I recommend fermented dairy foods as part of your dairy intake. That’s a recommendation everyone can agree with!
- One recent study has suggested that diet context is important. Specifically, the study suggests that the benefits of full-fat dairy foods are greatest in the context of a healthy, primarily plant-based diet.
-
- Similar observations have been made for egg consumption. That suggests that full-fat dairy and eggs provide some important nutrients that may be missing in a vegetarian diet. But in a diet that is already high in saturated fat and cholesterol, the “bad” effects of full-fat dairy and eggs may outweigh the benefits.
You can find more information about full-fat dairy by going to https://www.chaneyhealth.com/healthtips/ and putting “dairy” in the search box.
As for the amount of dairy foods you should consume, I wouldn’t get hung up on the number of servings per day. I interpret the new guidelines as saying, “Don’t be afraid of dairy. It can be an important part of your diet.”
However, the servings of dairy products are more frequently determined by lactose intolerance or sensitivity to milk protein than by dietary guidelines. Many people, including myself, can only consume small, occasional servings of dairy without experiencing digestive distress.
#4: Eat Vegetables & Fruits Throughout The Day
 The dietary guidelines say, “Eat a variety of colorful, nutrient-dense vegetables and fruits. Specifically, the recommendation is:
The dietary guidelines say, “Eat a variety of colorful, nutrient-dense vegetables and fruits. Specifically, the recommendation is:
- 3 servings/day of vegetables and 2 servings/day of fruits each day.
-
- Once again, the number of servings are based on a 2,000-calorie diet.
-
- When you take into account the actual caloric intake of Americans, the recommendations become 3-5 servings/day of vegetables and 2-4 servings/day of fruits.
These recommendations are not controversial. They are universally accepted.
#5: Incorporate Healthy Fats
The new dietary guidelines are:
- “Healthy fats are plentiful in many whole foods, such as meats, poultry, eggs, omega-3 rich seafood, nuts, seeds, full-fat dairy, olives, and avocados.”
-
- This recommendation is not controversial.
- “When cooking with or adding fats to meals, prioritize oils with essential fatty acids, such as olive oil. Other options can include butter or beef tallow.”
-
- This is the most controversial portion of the new dietary guidelines. The usual comment is something like, “How dare they include butter and lard as healthy fats!”
I’m not a fan of lard but let me make a couple of observations about butter.
- Butter is a whole food. Its ingredient list is typically cream, milk, and salt. If you buy the unsalted version, the ingredient list is even shorter. Margarine and butter substitutes have much longer ingredient lists, often including some questionable ingredients.
- The frequency of butter use is important. Let me share a personal example. We eat a whole food, primarily plant-based diet. We substitute almond butter for butter on toast and muffins. But there are certain foods like potatoes, winter squash, and corn on the cob that just aren’t the same without real butter. We buy 4 sticks of butter at a time, cut it into pats of butter, and freeze it. Four sticks of butter lasts us a year.
Finally, the critics who say that the new guidelines should not include foods that are high in saturated fat are ignoring the fact that the guidelines say, “Saturated fat consumption should not exceed 10% of total daily calories.” This statement has remained constant since the first food guide pyramid in 1992.
So, the new guidelines are not recommending that we eat more saturated fat as many critics have claimed. They are saying, “A little bit of saturated fat is OK in the context of a whole food diet with lots of fruits, vegetables, and whole grains.
#6: Focus On Whole Grains
 The new dietary guidelines are:
The new dietary guidelines are:
- “Prioritize fiber-rich whole grains.”
- “Significantly reduce the consumption of highly processed, refined carbohydrates.”
These guidelines are unchanged from previous versions of the guidelines.
What is new is that the guidelines now recommend only 2-4 servings of whole grains per day. That’s a big change from the 6-11 servings per day recommended in the original food guide pyramid.
- If the 6-11 servings per day were whole grains, the new recommendation would represent a significant decrease in fiber intake. But that’s not how most Americans eat.
- Since most of the grains in a typical American’s diet are highly processed and refined, reducing the recommended intake to 2-4 servings per day is a step in the right direction.
#7: Limit Highly Processed Foods, Added Sugars, & Refined Carbohydrates
 I call this, “Avoid the bad stuff”. Specifically:
I call this, “Avoid the bad stuff”. Specifically:
- Avoid highly processed foods with added sugar and sodium.
- Limit foods and beverages that include artificial flavors, colors, preservatives, and sweeteners
- Avoid sugar-sweetened and artificially sweetened beverages.
These recommendations are accepted by almost everyone except the food industry.
However, I should point out that there is also a slight difference in emphasis from previous versions of the USDA dietary guidelines:
- The new guidelines are more restrictive for added sugars than previous versions of the dietary guidelines. For example, they say:
-
- One meal should contain no more than 10 grams of added sugars.
-
- Children under the age of 10 should not be given foods with added sugars (previous versions of the dietary guidelines recommend avoiding added sugars for children under the age of 2).
Given the wealth of evidence that added sugars are linked to increased risk of obesity and chronic diseases, these stricter restrictions on added sugars make good sense – especially because the USDA dietary guidelines form the basis for school lunch programs.
But these guidelines are very different from how the average American eats. I’m not sure how many Americans will follow them.
#8: Limit Alcoholic Beverages
 The guidelines:
The guidelines:
- Say, “Consume less alcohol for better overall health”.
- List people who should completely avoid alcohol.
The only controversy about this recommendation is that it is less specific than the previous guidelines that recommended no more than 1 alcoholic drink/day for women and no more than 2/day for men.
I recognize the desire for specificity. But alcohol tolerance depends on several factors such as body weight, genetics, and medication usage.
What Does This Mean For You?
 The USDA just released a new version of the Food Guide Pyramid and accompanying “Dietary Guidelines For Americans”, and they are very different from previous versions. What do these changes mean for you?
The USDA just released a new version of the Food Guide Pyramid and accompanying “Dietary Guidelines For Americans”, and they are very different from previous versions. What do these changes mean for you?
While the AMA and AHA have both endorsed the new guidelines, they have been controversial. In the article above, I have summarized the pros and cons of every recommendation. There are lots of recommendations, so it was a long article.
To help you make sense of the article let me summarize the recommendations and criticisms by dividing the recommendations into 4 categories:
#1: Recommendations that are accepted by almost everyone except the food industry. These are non-controversial.
- Eat real food
- Eat vegetables and fruits throughout the day.
- Focus on whole grains.
- Limit highly processed foods, added sugar, and refined carbohydrates.
#2: Changes in recommendations that reflect recent scientific advances. Critics of these changes simply haven’t kept up with scientific publications over the past couple of decades.
- Increasing the daily protein recommendations.
- Including full-fat dairy as a healthy dairy food.
#3: Tempests in a teapot: There is a kernel of truth in these criticisms, but the changes are much more modest than the critics would have you believe.
- Including red meat in the protein recommendations.
- Including some saturated fats in the “healthy fats” category.
- Not including specific limits on alcohol consumption, as the previous version had done.
#4: What I would have liked to have seen:
- More emphasis on plant proteins.
- Elimination of lard from the “healthy fat” category.
- Inclusion of high-quality vegetable oils in the “healthy fats” category.
The Bottom Line
The USDA just released a new version of the Food Guide Pyramid and accompanying “Dietary Guidelines For Americans”.
While the AMA and AHA have both endorsed the new guidelines, they have been controversial.
In this article I describe the pros and cons of each dietary guideline and divide them into ones for which:
- They are clearly an improvement over the previous guideline.
- They are accepted by almost everyone.
- The criticism is a “tempest in a teapot”.
- The criticism is at least partially accurate.
For more information on the pros and cons of the new “Dietary Guidelines For Americans” and how these guidelines apply to you, read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure or prevent any disease.
_____________________________________________________________________________
My posts and “Health Tips From the Professor” articles carefully avoid claims about any brand of supplement or manufacturer of supplements. However, I am often asked by representatives of supplement companies if they can share them with their customers.
My answer is, “Yes, as long as you share only the article without any additions or alterations. In particular, you should avoid adding any mention of your company or your company’s products. If you were to do that, you could be making what the FTC and FDA consider a “misleading health claim” that could result in legal action against you and the company you represent.
For more detail about FTC regulations for health claims, see this link.
https://www.ftc.gov/business-guidance/resources/health-products-compliance-guidance
_______________________________________________________________________
About The Author
 Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years. Dr. Chaney won numerous teaching awards at UNC, including the Academy of Educators “Excellence in Teaching Lifetime Achievement Award”. Dr Chaney also ran an active cancer research program at UNC and published over 100 scientific articles and reviews in peer-reviewed scientific journals. In addition, he authored two chapters on nutrition in one of the leading Biochemistry textbooks for medical students.
Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years. Dr. Chaney won numerous teaching awards at UNC, including the Academy of Educators “Excellence in Teaching Lifetime Achievement Award”. Dr Chaney also ran an active cancer research program at UNC and published over 100 scientific articles and reviews in peer-reviewed scientific journals. In addition, he authored two chapters on nutrition in one of the leading Biochemistry textbooks for medical students.
Since retiring from the University of North Carolina, he has been writing a weekly health blog called “Health Tips From the Professor”. He has also written two best-selling books, “Slaying the Food Myths” and “Slaying the Supplement Myths”. And most recently he has created an online lifestyle change course, “Create Your Personal Health Zone”. For more information visit https://chaneyhealth.com.
For the past 55 years Dr. Chaney and his wife Suzanne have been helping people improve their health holistically through a combination of good diet, exercise, weight control and appropriate supplementation.