The Effect Of Ultra-Processed Foods On Heart Disease Risk
Author: Dr. Stephen Chaney
 Heart disease is a killer. It continues to be the leading cause of death – both worldwide and in industrialized countries like the United States and the European Union. When we look at heart disease trends, it is a good news – bad news situation.
Heart disease is a killer. It continues to be the leading cause of death – both worldwide and in industrialized countries like the United States and the European Union. When we look at heart disease trends, it is a good news – bad news situation.
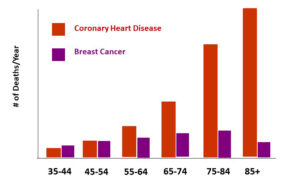
- The good news is that heart disease deaths are continuing to decline in adults over 70.
-
- The decline among senior citizens is attributed to improved treatment of heart disease and more seniors following heart-healthy diets.
- The bad news is that heart disease deaths are starting to increase in younger adults, something I reported in an earlier issue of “Health Tips From the Professor.”
-
- The reason for the rise in heart disease deaths in young people is less clear. However, the obesity epidemic, junk and convenience foods, and the popularity of fad diets all likely play a role.
Everyone has a magic diet to reduce the risk of heart disease. The American Heart Association tells us to avoid fats, especially saturated fats. Vegans tell us to avoid animal protein. Paleo and Keto enthusiasts tell us carbs are the problem.
But what if we eliminated junk and convenience food AND switched to a really healthy diet? How much would that reduce heart disease risk? A recent study (Y Willett et al, The American Journal of Medicine, in press, 2026) looked at the first part of that question. It looked at the effect of ultra-processed food (what we call junk and convenience foods) consumption on the risk of developing heart disease.
How Was This Study Done?
 The scientists analyzed data from 4787 participants in the most recently published (2021 to 2023) National Health and Nutrition Examination Survey (NHANES). The average age of participants in the survey was 55 years, with 56% of them being women.
The scientists analyzed data from 4787 participants in the most recently published (2021 to 2023) National Health and Nutrition Examination Survey (NHANES). The average age of participants in the survey was 55 years, with 56% of them being women.
All the participants in this study had completed a dietary survey of everything they ate over the last two days. They also reported whether they had ever experienced a heart attack or stroke.
Ultra-processed foods were defined as foods that are industrially modified and loaded with added fats, sugars, starches, salts, and chemical additives.
The percentage of ultra-processed foods in their diet was calculated, and the participants were divided into quartiles based on the percentage of ultra-processed foods they consumed.
Participants with the highest quartile of ultra-processed food consumption were compared to those in the lowest quartile with respect to the risk of cardiovascular disease (self-reported heart attack or stroke). The data were corrected for age, sex, race, ethnicity, smoking status, and income.
The Effect Of Ultra-Processed Foods On Heart Disease Risk
 The results were striking:
The results were striking:
- The participants in the highest quartile for ultra-processed food consumption had a 47% higher risk of heart disease compared to those in the lowest quartile for ultra-processed food consumption.
The authors concluded, “Adults who consumed the highest amount of ultra-processed foods had a statistically significant 47% increased risk of heart disease. Large scale randomized trials are needed, but in the meantime, health care providers should advise patients to decrease consumption of ultra-processed foods in addition to adopting other therapeutic lifestyle changes and adjunctive drug therapies of proven benefit.”
The authors recognized the difficulty of making those changes in a world where ultra-processed foods are ubiquitous and cheap.
However, they drew parallels to tobacco use in this country. They said, “Just as it took decades for the dangers of smoking to become widely accepted, reducing reliance on ultra-processed foods may take time. This is partly due to the influence of large multinational companies that dominate the food market. In addition, many people face limited access to healthier food options.”
They went on to say, “Addressing ultra-processed foods isn’t just about individual choices – it’s about creating environments where the healthy option is the easy option.”
Can You Cut Your Risk Of Heart Disease By 90%?
 The short answer is, “probably not”. But you can reduce the risk of heart disease by a lot – and probably by a lot more than 47%.
The short answer is, “probably not”. But you can reduce the risk of heart disease by a lot – and probably by a lot more than 47%.
That’s because this study did not look at what the participants were replacing the ultra-processed foods with. Some participants may have replaced them with whole food, primarily plant-based diets. Others may have replaced ultra-processed foods with whole food, meat-based diets high in saturated fats.
So, let’s look at the other side of the equation – how much you can reduce your risk of heart disease by eating a healthier diet. In a recent issue of “Health Tips From The Professor”, I reviewed a meta-analysis published in 2022 that looked at 99 clinical studies with tens of thousands of participants that measured the associations between foods or food groups and heart disease risk.
That study reported that:
- Processed Meat: A single serving of processed meat increased heart disease risk by 27% to 44%.
- Red Meat: Unprocessed red meat increased heart disease risk by as much as 27% – but only at ≥3 servings per day. The results with lower intakes were inconsistent – some studies showed increased risk, but others did not.
- Poultry, Eggs, and Dairy Foods: They did not appear to affect heart disease risk.
- Fish: Two to four servings per week of fatty fish decreased heart disease risk by around 12%.
- Fruit: Two servings per day of fruit reduced heart disease risk by 21-32%.

- Vegetables: Two servings of vegetables per day reduced heart disease risk by 18-21%.
- Legumes (beans and peas): Four servings per week reduced the risk of heart disease by around 14%.
- Nuts: One serving (a handful) per day reduced the risk of heart disease by around 25%.
- Whole Grains: Two servings of whole grains per day reduced the risk of heart disease by 25%-34%.
- Overall: When heart-healthy foods were consumed as part of the Mediterranean diet heart disease risk was reduced by 47%. Similar overall reductions in heart disease risk are likely with other heart-healthy diets like DASH, MIND, Flexitarian (flexible semi-vegetarian), and vegan diets.
In summary:
- The first study shows that eliminating ultra-processed foods (junk and convenience foods) from your diet can decrease heart disease risk by 47% – but doesn’t tell us what the ultra-processed foods were replaced with. And it would take a much larger study to determine which food swaps were most effective at reducing heart disease risk.
- The second study was a meta-analysis that told us that eating more fish and plant foods in the context of a heart-healthy diet can decrease your risk of heart disease by 47% – but doesn’t tell us what those healthy foods were replacing. And many of the individual studies included in the meta-analysis were conducted when ultra-processed food consumption was much less than it is today.
It would be tempting to add 47% plus 47% and conclude that eliminating ultra-processed food consumption and replacing ultra-processed foods with heart-healthy foods could decrease your risk of heart disease by 94%. But it’s not that simple. There are too many unanswered questions from these studies.
But it is safe to say that if we eliminated ultra-processed foods AND replaced them with heart-healthy foods in the context of a heart-healthy diet, we should be able to reduce our heart disease risk by more than 47% – perhaps much more.
What Do These Studies Mean For You?
 There are two important lessons from these studies:
There are two important lessons from these studies:
#1: Eliminating ultra-processed foods from your diet will significantly decrease your risk of heart disease.
And it isn’t just heart disease. Other recent studies have shown that eliminating ultra-processed foods from your diet helps you:
- Control your weight (It is perhaps the most important lifestyle change to make if you want to maintain GLP-1-aided weight loss).
- Reduce your risk of cancer.
- Reduce your risk of diabetes.
- Reduce your risk of inflammatory diseases.
- Reduce anxiety and depression.
- Increase your healthspan (your healthy years).
In short, ultra-processed foods are killers.
#2: Replacing ultra-processed foods with heart-healthy foods (fruits, vegetables, legumes, nuts, whole grains, and fish) in the context of a healthy diet (Mediterranean, DASH, MIND, Flexitarian, and vegan, for example) is likely to decrease your risk of heart disease even more.
- And if your diet consists of mostly heart-healthy foods, you can add moderate amounts of heart-neutral foods (poultry, eggs, and dairy).
- And the latest evidence suggests that you can even add small amounts of red meat in the context of a heart-healthy diet (As I have said in previous issues of “Health Tips From the Professor”, plant foods contain the antidotes to all the bad things about red meat.)
Finally, you might ask why I emphasize both heart-healthy foods and heart-healthy diets. There are two reasons:
- Most of us think in terms of foods rather than diets.
- The food industry is only too happy to provide us with ultra-processed foods for “heart-healthy” diets like the vegan and Mediterranean diet.
The Bottom Line
Two recent studies have shown how each of us can dramatically reduce our risk of heart disease.
- The first study showed that eliminating ultra-processed foods from our diet can significantly decrease our heart disease risk – but didn’t tell us what the ultra-processed foods were replaced with.
- The second study showed that eating more heart-healthy foods in the context of a heart-healthy diet can significantly decrease our risk of heart disease – but didn’t tell us what those healthy foods were replacing.
Taken together, those studies show us a clear path for dramatically decreasing our heart disease risk.
For more details about these studies and what they mean for you, read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure or prevent any disease.
_____________________________________________________________________________
My posts and “Health Tips From the Professor” articles carefully avoid claims about any brand of supplement or manufacturer of supplements. However, I am often asked by representatives of supplement companies if they can share them with their customers.
My answer is, “Yes, as long as you share only the article without any additions or alterations. In particular, you should avoid adding any mention of your company or your company’s products. If you were to do that, you could be making what the FTC and FDA consider a “misleading health claim” that could result in legal action against you and the company you represent.
For more detail about FTC regulations for health claims, see this link.
https://www.ftc.gov/business-guidance/resources/health-products-compliance-guidance
_______________________________________________________________________
About The Author
 Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years. Dr. Chaney won numerous teaching awards at UNC, including the Academy of Educators “Excellence in Teaching Lifetime Achievement Award”.
Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years. Dr. Chaney won numerous teaching awards at UNC, including the Academy of Educators “Excellence in Teaching Lifetime Achievement Award”.
Dr Chaney also ran an active cancer research program at UNC and published over 100 scientific articles and reviews in peer-reviewed scientific journals. In addition, he authored two chapters on nutrition in one of the leading biochemistry text books for medical students.
Since retiring from the University of North Carolina, he has been writing a weekly health blog called “Health Tips From the Professor”. He has also written two best-selling books, “Slaying the Food Myths” and “Slaying the Supplement Myths”. And most recently he has created an online lifestyle change course, “Create Your Personal Health Zone”. For more information visit https://chaneyhealth.com.
For the past 45 years Dr. Chaney and his wife Suzanne have been helping people improve their health holistically through a combination of good diet, exercise, weight control and appropriate supplementation.